Department of Psychiatry, University of Maryland Medical Center and Sheppard Pratt Health System, Baltimore, Maryland, USA.
Clinical Research, Sheppard Pratt Health System, Baltimore, Maryland, USA.
Brain Behav. 2020 Dec;10(12):e01805. doi: 10.1002/brb3.1805. Epub 2020 Nov 10.
Treatment options are limited for patients with bipolar depression. Antidepressants added to mood stabilizers even carry risks of precipitating mixed/manic episodes. Transcranial magnetic stimulation (TMS) may provide a safe and effective option for these patients.
Database analysis of the TMS Service at Sheppard Pratt Health System identified patients with bipolar disorder type I (BD1) or II (BD2) in a pure depressive phase at initiation of TMS. Records were reviewed for response and remission rates based on MADRS scores, time to effect, and adverse events, notably treatment-emergent affective switching. All had failed at least two prior treatments for depression, were currently on at least one mood stabilizer and off antidepressants. Stimulation parameters targeted left dorsolateral prefrontal cortex: 120% motor threshold, 10 pulses per second (pps) × 4s, intertrain interval (ITI) 26s, 75 trains (37.5 min/session) for 3,000 pps total, 5 sessions/week for 30 total treatments, or until remission criteria were met.
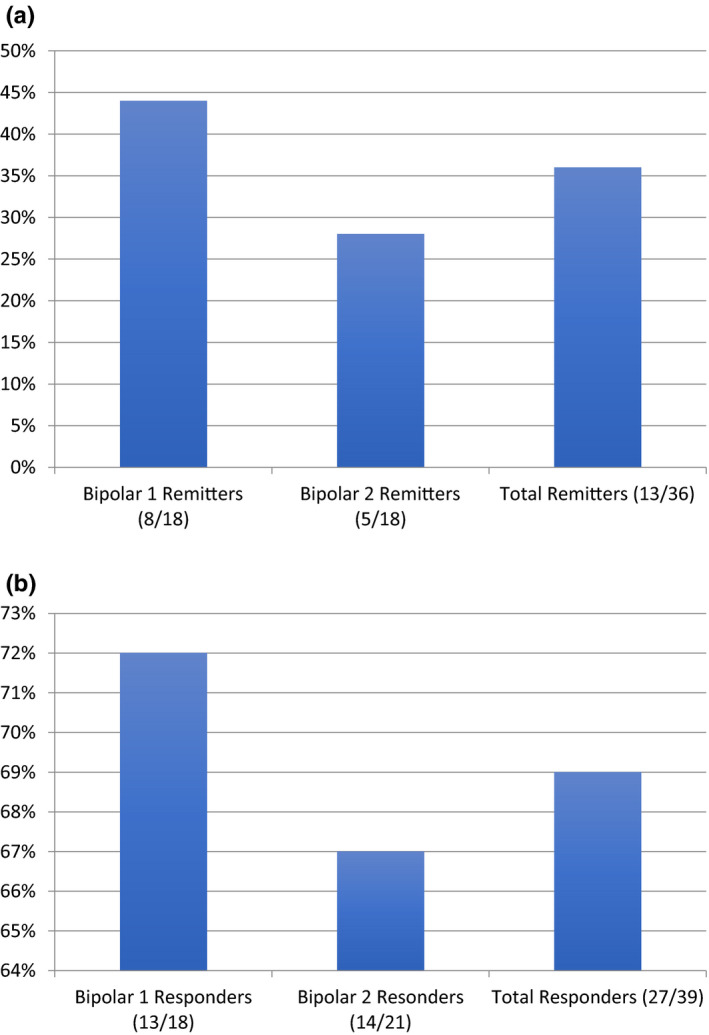
A total of 44 patients with BD were identified, representing 15% of the total TMS population. 77% of those who completed a course of TMS met response criteria, and 41% of subjects who completed at least 25 treatments met remission criteria. Subjects with BD1 were more likely to respond, remit, or suffer an adverse event than those with BD2. No patient met clinical criteria for a manic/mixed episode, but four (10%) discontinued due to concerns of activation.
TMS is effective in the bipolar depressed population where episode focused intervention can be specifically offered. Risk of psychomotor agitation must be closely monitored.
对于双相情感障碍患者的治疗选择有限。即使在心境稳定剂的基础上添加抗抑郁药,也可能带来诱发混合/躁狂发作的风险。经颅磁刺激(TMS)可能为这些患者提供一种安全有效的选择。
对 Sheppard Pratt 健康系统 TMS 服务的数据库进行分析,确定在开始 TMS 时处于单相抑郁期的 I 型(BD1)或 II 型(BD2)双相情感障碍患者。根据 MADRS 评分、起效时间和不良反应(尤其是治疗诱发的情感转换),评估患者的反应和缓解率。所有患者均在接受至少两种先前的抗抑郁治疗后失败,目前至少服用一种心境稳定剂且停用抗抑郁药。刺激参数针对左背外侧前额叶皮质:120%运动阈值,每秒 10 脉冲(pps)×4 秒,每个训练周期之间的间隔(ITI)为 26 秒,75 个训练周期(37.5 分钟/次)共 3000 个脉冲,每周 5 次,共 30 次治疗,或直至达到缓解标准。
共确定了 44 例双相情感障碍患者,占 TMS 总人数的 15%。完成 TMS 疗程的患者中,77%符合反应标准,完成至少 25 次治疗的患者中,41%符合缓解标准。与 BD2 患者相比,BD1 患者更有可能出现反应、缓解或发生不良反应。没有患者符合躁狂/混合发作的临床标准,但有 4 例(10%)因担心激活而停止治疗。
TMS 对双相抑郁患者有效,可提供针对发作的干预措施。必须密切监测精神运动兴奋的风险。