Tong Jia Wei Valerie, Lingam Pravin, Shelat Vishalkumar Girishchandra
Yong Loo Lin School of Medicine National University of Singapore Singapore Singapore.
Department of General Surgery Tan Tock Seng Hospital Singapore Singapore.
Acute Med Surg. 2020 Nov 4;7(1):e587. doi: 10.1002/ams2.587. eCollection 2020 Jan-Dec.
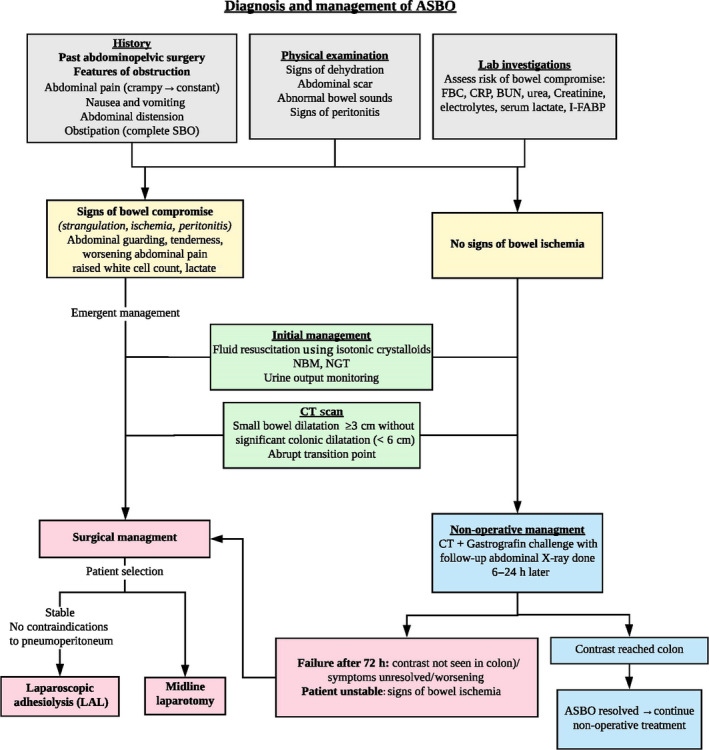
Small bowel obstruction (SBO) accounts for 12-16% of emergency surgical admissions and 20% of emergency surgical procedures. Even with the advent of laparoscopic surgery, intra-abdominal adhesions remain a significant cause of SBO, accounting for 65% of cases. History and physical examination are essential to identify signs of bowel ischemia as this indicates a need for urgent surgical exploration. Another critical aspect of evaluation includes establishing the underlying cause for obstruction and distinguishing between adhesive and non-adhesive etiologies as adhesive SBO (ASBO) can be managed non-operatively in 70-90% of patients. A patient with a history of abdominopelvic surgery along with one or more cardinal features of obstruction should be suspected to have ASBO until proven otherwise. Triad of severe pain, pain out of proportion to the clinical findings, and presence of an abdominal scar suggest possible closed-loop obstruction. Computed tomography has higher sensitivity and specificity compared to plain films and is recommended by the Bologna guidelines. Correcting fluid and electrolyte imbalance is an initial crucial step to mitigate severe hypovolemia. Patients should proceed with surgery if symptoms of bowel compromise are present, or if symptoms do not resolve or have worsened. Surgery is indicated in patients with ischemia, strangulation, perforation, peritonitis, or failure of non-operative treatment. With advances in minimal access technology and increasing experience, laparoscopic adhesiolysis is recommended. Mechanical adhesion barriers are an effective measure to prevent adhesion formation.
小肠梗阻(SBO)占急诊外科入院病例的12% - 16%,以及急诊外科手术的20%。即使腹腔镜手术问世,腹腔内粘连仍是SBO的重要原因,占病例的65%。病史和体格检查对于识别肠缺血迹象至关重要,因为这表明需要紧急进行手术探查。评估的另一个关键方面包括确定梗阻的潜在原因,并区分粘连性和非粘连性病因,因为70% - 90%的粘连性SBO(ASBO)患者可以采用非手术治疗。有腹部盆腔手术史且伴有一项或多项梗阻主要特征的患者,在未证实其他情况之前应怀疑患有ASBO。严重疼痛、疼痛程度与临床表现不符以及腹部有瘢痕三联征提示可能存在闭环梗阻。与平片相比,计算机断层扫描具有更高的敏感性和特异性,博洛尼亚指南推荐使用。纠正液体和电解质失衡是减轻严重血容量不足的首要关键步骤。如果出现肠功能受损症状,或者症状未缓解或加重,患者应进行手术。对于有缺血、绞窄、穿孔、腹膜炎或非手术治疗失败的患者,需进行手术。随着微创技术的进步和经验的增加,推荐进行腹腔镜粘连松解术。机械性粘连屏障是预防粘连形成的有效措施。