Rohani Pejman, Karimi Abdollah, Tabatabaie Sedigheh Rafiei, Khalili Mitra, Sayyari Aliakbar
Pediatric Gastroenterology, Hepatology and Nutrition Research Center, Research Institute of Children Health, Shahid Beheshti University of Medical Sciences, Shariati Ave, Infront of Hoseinieh Ershad, Tehran, Iran.
Pediatric Infectious Research Center, Research Institute of Children Health, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
J Pediatr Surg Case Rep. 2021 Jan;64:101667. doi: 10.1016/j.epsc.2020.101667. Epub 2020 Nov 5.
Severe acute respiratory syndrome corona virus 2 (SARS- CoV-2) is known as COVID 19 seems to be one of the most contagious and dangerous infection in children and adults. According to first adult studies association of gastrointestinal (GI) symptoms with COVID 19 infection was as high as 79% (1).But later study showed lower association around 18% (2).As the pandemic of COVID 19 is going on, different clinical presentation of disease especially in children are well appeared. In addition atypical presentations may confuse and mislead physician to do different diagnostic procedures and interventions. We report a 6 years and half old boy with diarrhea, abdominal pain with first diagnosis acute abdomen due to acute appendicitis. At last diagnosis of pneumatosis intestinalis due to enterocolitis was confirmed.
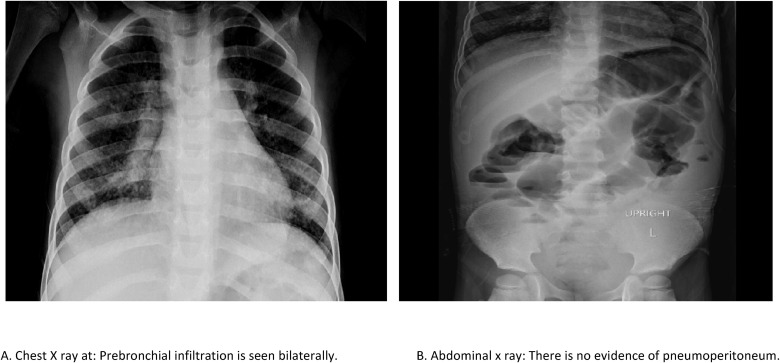
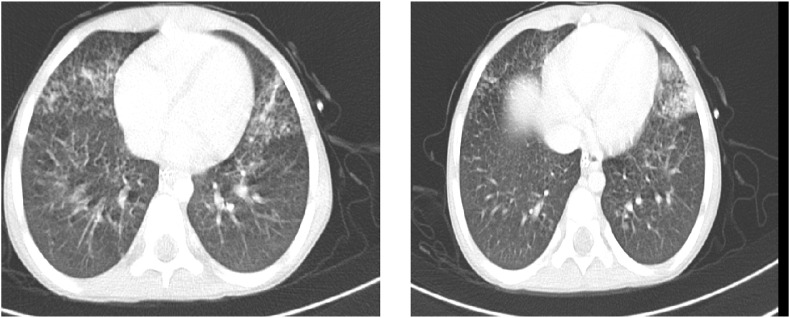
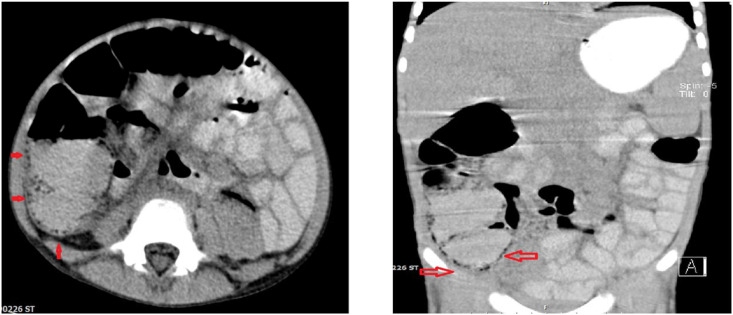
A 6 years and half old boy with severe abdominal pain admitted in emergency ward. He had history of fever, nine days of diarrhea and recurrent vomiting. The abdominal pain was severe with moderate tenderness in right lower quadrant. He admitted in pediatric surgery ward after surgical consultation for rolling out acute appendicitis. The results of first lab studies were shown leucopenia, lymphopenia and COVID 19 PCR was positive. During admission the cough has increased and abdominal distention has evolved. Vomiting was intractable and feeding was impossible. Pneumatosis intestinalis in ascending colon and dilatation in colon caliber were detected abdominal. Miliary like pattern in lung has reported in chest CT. Stool exam results revealed loss of protein in high amount in spite of normal pancreatic and enterocyte function. The calprotectin was high and implied high inflammation in large intestine. With all above data necrotizing enterocolitis management was started. After 14 days patients had good appetite and feeding slowly introduced. All symptoms resolved with exception of cough. Albumin and other electrolytes remained stable. The patient discharged without morbidity.
COVID 19 infection has many different and mysterious presentations. GI manifestations are among important, common presentations. The acute abdomen like presentation with different complications like pneumatosis intestinalis, protein losing enteropathy are not common but knowledge about these presentations assist physician to be aware and make decision accurately.
严重急性呼吸综合征冠状病毒2(SARS-CoV-2)引发的疾病被称为COVID-19,似乎是儿童和成人中传染性最强、最危险的感染之一。根据最初针对成人的研究,胃肠道(GI)症状与COVID-19感染的关联高达79%(1)。但后来的研究显示该关联较低,约为18%(2)。随着COVID-19大流行的持续,该疾病的不同临床表现,尤其是在儿童中的表现愈发明显。此外,非典型表现可能会使医生困惑并误导其进行不同的诊断程序和干预措施。我们报告一名6岁半的男孩,最初因急性阑尾炎被诊断为急腹症,伴有腹泻和腹痛。最终确诊为因小肠结肠炎导致的肠壁积气。
一名6岁半的男孩因严重腹痛入住急诊病房。他有发热、九天腹泻和反复呕吐的病史。腹痛严重,右下腹有中度压痛。经外科会诊以排除急性阑尾炎后,他被收入小儿外科病房。首次实验室检查结果显示白细胞减少、淋巴细胞减少,且COVID-19聚合酶链反应呈阳性。住院期间咳嗽加重,腹胀加剧。呕吐难以控制,无法进食。腹部检查发现升结肠有肠壁积气,结肠管径增宽。胸部CT报告肺部有粟粒样病变。粪便检查结果显示尽管胰腺和肠细胞功能正常,但蛋白质大量流失。钙卫蛋白升高,提示大肠有高度炎症。基于上述所有数据,开始进行坏死性小肠结肠炎的治疗。14天后,患者食欲良好,开始缓慢进食。除咳嗽外,所有症状均已缓解。白蛋白和其他电解质保持稳定。患者出院,无并发症。
COVID-19感染有许多不同且神秘的表现。胃肠道表现是重要且常见的表现之一。类似急腹症的表现以及诸如肠壁积气、蛋白丢失性肠病等不同并发症并不常见,但了解这些表现有助于医生提高认识并准确做出决策。