Chen Shixue, Huang Ziwei, Jia Wangping, Tao Haitao, Zhang Sujie, Ma Junxun, Liu Zhefeng, Wang Jinliang, Wang Lijie, Cui Pengfei, Zhang Zhibo, Huang Di, Wu Zhaozhen, Zheng Xuan, Hu Yi
Department of Graduate Administration, Chinese PLA General Hospital, Beijing, People's Republic of China.
Department of Medical Oncology, Chinese PLA General Hospital, Beijing, People's Republic of China.
J Hepatocell Carcinoma. 2020 Nov 2;7:289-299. doi: 10.2147/JHC.S277453. eCollection 2020.
At present, there are no validated biomarkers that can predict whether patients with advanced hepatocellular carcinoma (aHCC) are likely to benefit from anti-PD-1 therapy. We aimed to determine whether lung immune prognostic index (LIPI) is associated with outcomes in patients with aHCC treated with PD-1 inhibitors.
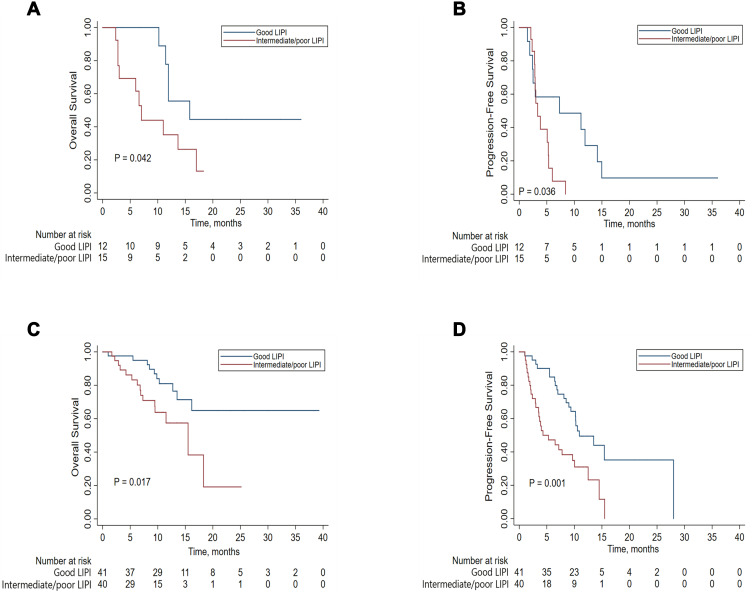
Patients undergoing initial treatment with PD-1 inhibitors for aHCC at a single center from January 1, 2015 to August 31, 2019 were included. The patients were stratified according to pretreatment LIPI based on a derived neutrophils/(leukocytes minus neutrophils) ratio (dNLR) ≥ 3 and a lactate dehydrogenase (LDH) level ≥ the upper limit of normal (ULN). Kaplan-Meier analysis and the Log rank test were used to calculate and compare survival between good LIPI and intermediate/poor LIPI scores. The prognostic values of LIPI for survival and disease control rate were evaluated using Cox proportional hazard and logistic regression models, respectively.
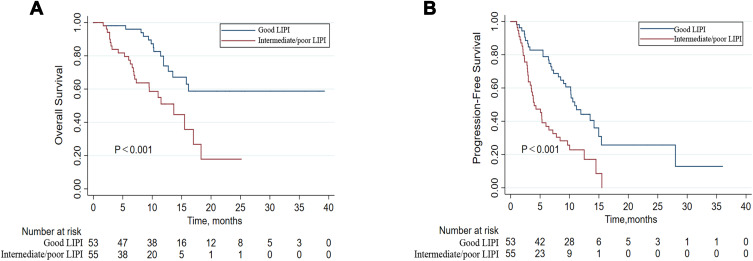
Of the 108 study patients, 53 (49%) had a good LIPI (dNLR < 3 and LDH normal) and 55 (51%) had intermediate/poor LIPI (dNLR ≥ 3 or/and LDH ≥ ULN). With a median follow-up of 12.4 months, intermediate/poor LIPI was independently associated with shorter overall survival (OS) (hazard ratio [HR] 4.00; 95% CI, 2.00-8.03) and progression-free survival (PFS) (HR 2.65; 95% CI, 1.61-4.37). The median OS for good and intermediate/poor LIPI was not reached and was 13.7 (95% CI, 8.2-19.1) months, respectively, and the median PFS was 10.9 (95% CI, 8.9-12.9) and 4.0 (95% CI, 2.2-5.8) months (both P < 0.001), respectively.
Pretreatment LIPI combined with a dNLR ≥ 3 and/or LDH ≥ ULN is associated with poor outcomes in patients with aHCC treated with PD-1 inhibitors. Further validation in large, prospective studies are warranted.
目前,尚无经过验证的生物标志物能够预测晚期肝细胞癌(aHCC)患者是否可能从抗PD-1治疗中获益。我们旨在确定肺免疫预后指数(LIPI)是否与接受PD-1抑制剂治疗的aHCC患者的预后相关。
纳入2015年1月1日至2019年8月31日在单一中心接受PD-1抑制剂初始治疗的aHCC患者。根据预处理LIPI进行分层,基于推导的中性粒细胞/(白细胞减去中性粒细胞)比值(dNLR)≥3和乳酸脱氢酶(LDH)水平≥正常上限(ULN)。采用Kaplan-Meier分析和Log rank检验计算并比较良好LIPI与中等/不良LIPI评分之间的生存率。分别使用Cox比例风险模型和逻辑回归模型评估LIPI对生存率和疾病控制率的预后价值。
108例研究患者中,53例(49%)LIPI良好(dNLR<3且LDH正常),55例(51%)LIPI中等/不良(dNLR≥3或/和LDH≥ULN)。中位随访12.4个月,中等/不良LIPI与较短的总生存期(OS)(风险比[HR]4.00;95%CI,2.00 - 8.03)和无进展生存期(PFS)(HR 2.65;95%CI,1.61 - 4.37)独立相关。良好和中等/不良LIPI的中位OS分别未达到和为13.7(95%CI,8.2 - 19.1)个月,中位PFS分别为10.9(95%CI,8.9 - 12.9)和4.0(95%CI,2.2 - 5.8)个月(均P<0.001)。
预处理LIPI联合dNLR≥3和/或LDH≥ULN与接受PD-1抑制剂治疗的aHCC患者的不良预后相关。有必要在大型前瞻性研究中进一步验证。