From the Department of Critical Care Medicine, University of Alberta.
Department of Anesthesiology & Critical Care Medicine, Saint Louis University.
Anesth Analg. 2021 Jun 1;132(6):1654-1665. doi: 10.1213/ANE.0000000000005250.
Intraoperative hypotension (IOH) occurs frequently during surgery and may be associated with organ ischemia; however, few multicenter studies report data regarding its associations with adverse postoperative outcomes across varying hemodynamic thresholds. Additionally, no study has evaluated the association between IOH exposure and adverse outcomes among patients by various age groups.
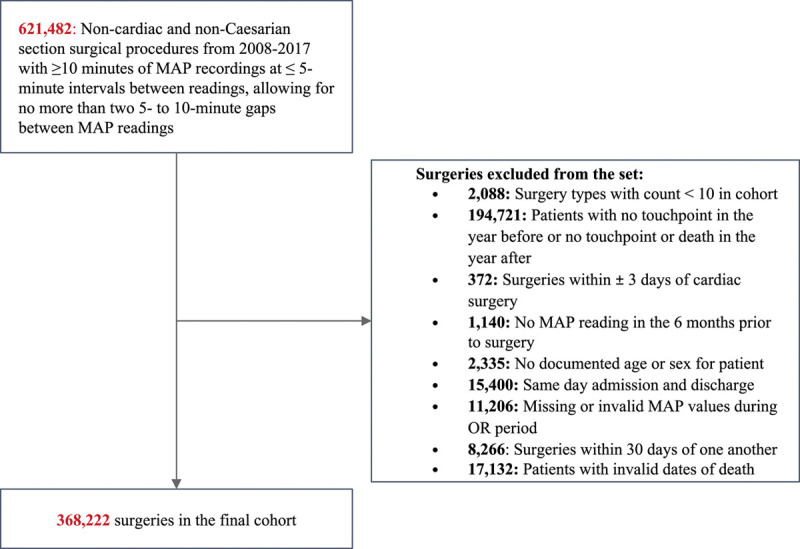
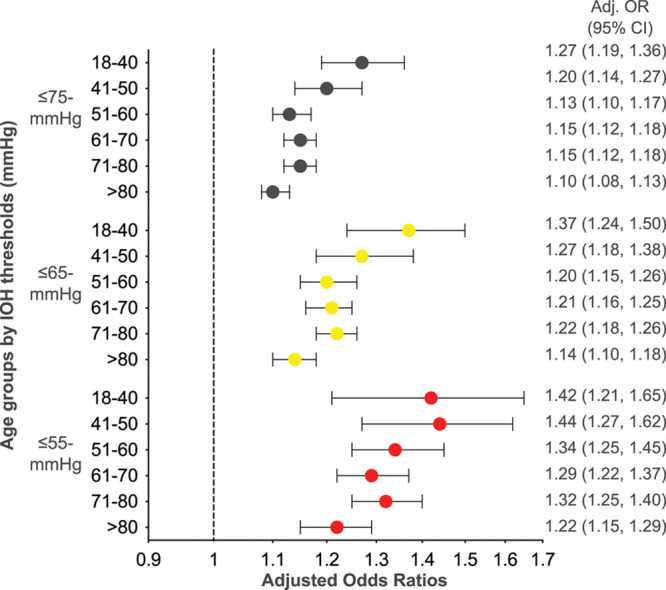
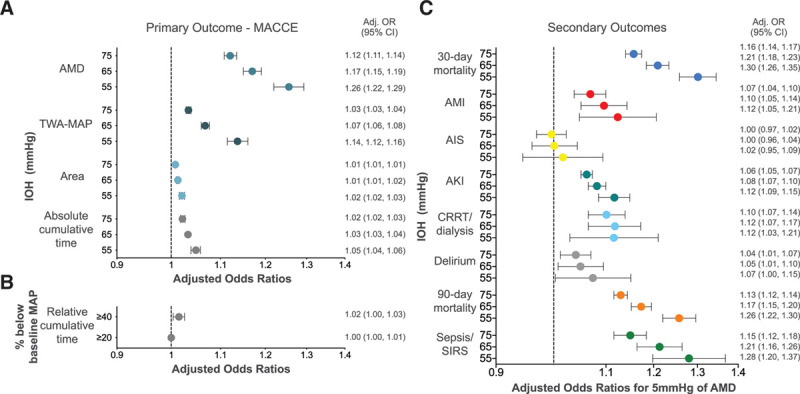
A multicenter retrospective cohort study was conducted between 2008 and 2017 using intraoperative blood pressure data from the US electronic health records database to examine postoperative outcomes. IOH was assessed in 368,222 noncardiac surgical procedures using 5 methods: (a) absolute maximum decrease in mean arterial pressure (MAP) during surgery, (b) time under each absolute threshold, (c) total area under each threshold, (d) time-weighted average MAP under each threshold, and (e) cumulative time under the prespecified relative MAP thresholds. MAP thresholds were defined by absolute limits (≤75, ≤65, ≤55 mm Hg) and by relative limits (20% and 40% lower than baseline). The primary outcome was major adverse cardiac or cerebrovascular events; secondary outcomes were all-cause 30- and 90-day mortality, 30-day acute myocardial injury, and 30-day acute ischemic stroke. Residual confounding was minimized by controlling for observable patient and surgical factors. In addition, we stratified patients into age subgroups (18-40, 41-50, 51-60, 61-70, 71-80, >80) to investigate how the association between hypotension and the likelihood of major adverse cardiac or cerebrovascular events and acute kidney injury differs in these age subgroups.
IOH was common with at least 1 reading of MAP ≤75 mm Hg occurring in 39.5% (145,743) of cases; ≤65 mm Hg in 19.3% (70,938) of cases, and ≤55 mm Hg in 7.5% (27,473) of cases. IOH was significantly associated with the primary outcome for all age groups. For an absolute maximum decrease, the estimated odds of a major adverse cardiac or cerebrovascular events in the 30-day postsurgery was increased by 12% (95% confidence interval [CI], 11-14) for ≤75 mm Hg; 17.0% (95% CI, 15-19) for ≤65 mm Hg; and by 26.0% (95% CI, 22-29) for ≤55 mm Hg.
IOH during noncardiac surgery is common and associated with increased 30-day major adverse cardiac or cerebrovascular events. This observation is magnified with increasing hypotension severity. The potentially avoidable nature of the hazard, and the extent of the exposed population, makes hypotension in the operating room a serious public health issue that should not be ignored for any age group.
术中低血压(IOH)在手术中经常发生,可能与器官缺血有关;然而,很少有多中心研究报告在不同的血流动力学阈值下与不良术后结果相关的数据。此外,尚无研究评估不同年龄组患者的 IOH 暴露与不良结局之间的关联。
使用美国电子健康记录数据库中的术中血压数据,进行了一项 2008 年至 2017 年的多中心回顾性队列研究,以检查术后结果。使用 5 种方法评估了 368222 例非心脏手术中的 IOH:(a)术中平均动脉压(MAP)的绝对最大下降,(b)每种绝对阈值下的时间,(c)每种阈值下的总面积,(d)每种阈值下的时间加权平均 MAP,以及(e)在预设的相对 MAP 阈值下的累积时间。MAP 阈值通过绝对限制(≤75、≤65、≤55mmHg)和相对限制(比基线低 20%和 40%)来定义。主要结局是主要心脏或脑血管不良事件;次要结局是全因 30 天和 90 天死亡率、30 天急性心肌损伤和 30 天急性缺血性卒中。通过控制可观察到的患者和手术因素,最大限度地减少残余混杂。此外,我们将患者分为年龄亚组(18-40 岁、41-50 岁、51-60 岁、61-70 岁、71-80 岁、>80 岁),以调查低血压与主要心脏或脑血管不良事件和急性肾损伤之间的关联在这些年龄亚组中的差异。
至少有 1 次 MAP≤75mmHg 的 IOH 很常见,占 39.5%(145743 例);MAP≤65mmHg 的占 19.3%(70938 例),MAP≤55mmHg 的占 7.5%(27473 例)。对于所有年龄组,IOH 与主要结局显著相关。对于绝对最大下降,30 天术后发生主要心脏或脑血管不良事件的估计几率增加了 12%(95%置信区间[CI],11-14),MAP≤75mmHg;17.0%(95% CI,15-19),MAP≤65mmHg;26.0%(95% CI,22-29),MAP≤55mmHg。
非心脏手术中的 IOH 很常见,与 30 天主要心脏或脑血管不良事件发生率增加有关。随着低血压严重程度的增加,这种观察结果更为明显。这种危害的潜在可避免性,以及暴露人群的范围,使得手术室内的低血压成为一个严重的公共卫生问题,任何年龄组都不应忽视。