Incorvaia Lorena, Fanale Daniele, Badalamenti Giuseppe, Porta Camillo, Olive Daniel, De Luca Ida, Brando Chiara, Rizzo Mimma, Messina Carlo, Rediti Mattia, Russo Antonio, Bazan Viviana, Iovanna Juan Lucio
Department of Biomedicine, Neuroscience and Advanced Diagnostics (Bi.n.d.), Section of Medical Oncology, University of Palermo, Palermo, Italy.
Department of Surgical, Oncological and Oral Sciences, Section of Medical Oncology, University of Palermo, Palermo, Italy.
Oncoimmunology. 2020 Oct 27;9(1):1832348. doi: 10.1080/2162402X.2020.1832348.
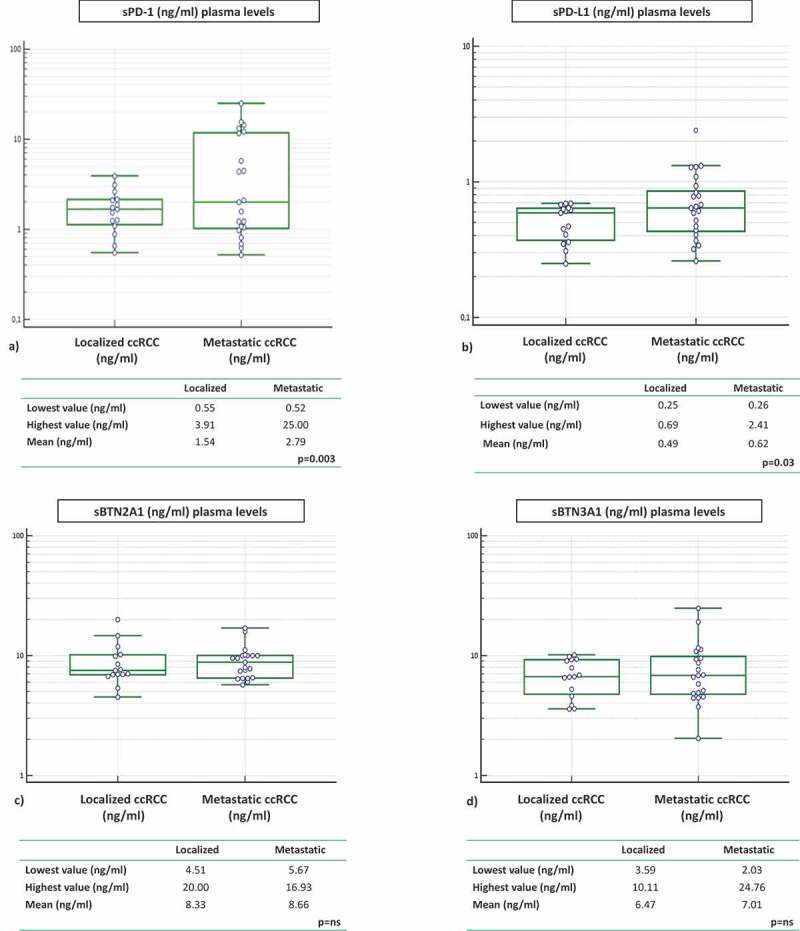
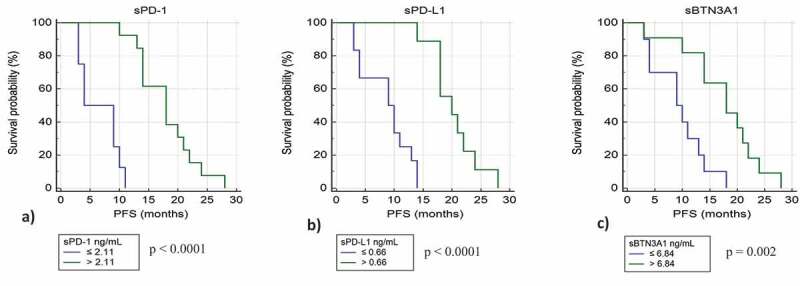
Despite a proportion of renal cancer patients can experiment marked and durable responses to immune-checkpoint inhibitors, the treatment efficacy is widely variable and identifying the patient who will benefit from immunotherapy remains an issue. We performed a prospective study to investigate if soluble forms of the immune-checkpoints PD-1 (sPD-1), PD-L1 (sPD-L1), pan-BTN3As, BTN3A1, and BTN2A1, could be candidate to predict the response to immune-checkpoint blockade therapy. We evaluated the plasma levels in a learning cohort of metastatic clear cell renal carcinoma (mccRCC) patients treated with the anti-PD-1 agent nivolumab by developed ELISA's. Using specific cut-offs determined through ROC curves, we showed that high baseline levels of sPD-1 (>2.11 ng/ml), sPD-L1 (>0.66 ng/ml), and sBTN3A1 (>6.84 ng/ml) were associated with a longer progression-free survival (PFS) to nivolumab treatment [median PFS, levels above thresholds: sPD-1, 20.7 months ( < .0001); sPD-L1, 19 months ( < .0001); sBTN3A1, 17.5 months ( = .002)]. High sPD-1 and sBTN3A1 levels were also associated with best overall response by RECIST and objective response of >20%. The results were confirmed in a validation cohort of 20 mccRCC patients. The analysis of plasma dynamic changes after nivolumab showed a statistically significant decrease of sPD-1 after 2 cycles (Day 28) in the long-responder patients. Our study revealed that the plasma levels of sPD-1, sPD-L1, and sBTN3A1 can predict response to nivolumab, discriminating responders from non-responders already at therapy baseline, with the advantages of non-invasive sample collection and real-time monitoring that allow to evaluate the dynamic changes during cancer evolution and treatment.
尽管一部分肾癌患者对免疫检查点抑制剂可产生显著且持久的反应,但治疗效果差异很大,确定哪些患者将从免疫治疗中获益仍是一个问题。我们进行了一项前瞻性研究,以调查免疫检查点PD-1(sPD-1)、PD-L1(sPD-L1)、泛BTN3A、BTN3A1和BTN2A1的可溶性形式是否可作为预测免疫检查点阻断治疗反应的指标。我们通过开发的酶联免疫吸附测定法(ELISA)评估了接受抗PD-1药物纳武单抗治疗的转移性透明细胞肾细胞癌(mccRCC)患者学习队列中的血浆水平。通过ROC曲线确定特定的临界值,我们发现sPD-1(>2.11 ng/ml)、sPD-L1(>0.66 ng/ml)和sBTN3A1(>6.84 ng/ml)的高基线水平与纳武单抗治疗的更长无进展生存期(PFS)相关[中位PFS,高于阈值水平:sPD-1,20.7个月(<.0001);sPD-L1,19个月(<.0001);sBTN3A1,17.5个月(=.002)]。高sPD-1和sBTN3A1水平也与根据实体瘤疗效评价标准(RECIST)的最佳总体反应以及>20%的客观反应相关。结果在20例mccRCC患者的验证队列中得到证实。纳武单抗治疗后血浆动态变化分析显示,长反应者患者在2个周期(第28天)后sPD-1有统计学显著下降。我们的研究表明,sPD-1、sPD-L1和sBTN3A1的血浆水平可预测对纳武单抗的反应,在治疗基线时就能区分反应者和无反应者,具有非侵入性样本采集和实时监测的优势,能够评估癌症进展和治疗期间的动态变化。