Spence J David
Neurology & Clinical Pharmacology, Western University, London, ON, Canada.
Stroke Prevention & Atherosclerosis Research Centre, Robarts Research Institute, London, ON, Canada.
Ann Transl Med. 2020 Oct;8(19):1262. doi: 10.21037/atm-20-975.
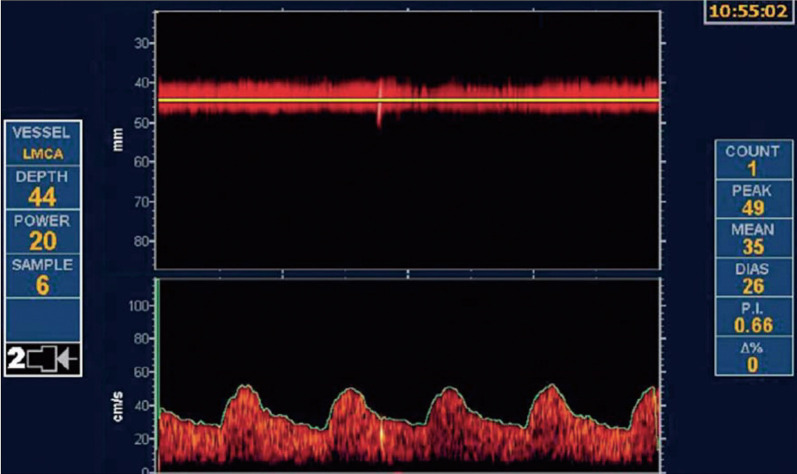
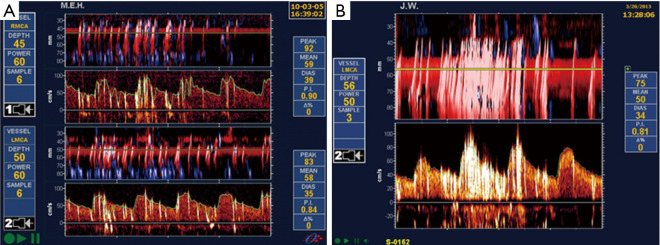
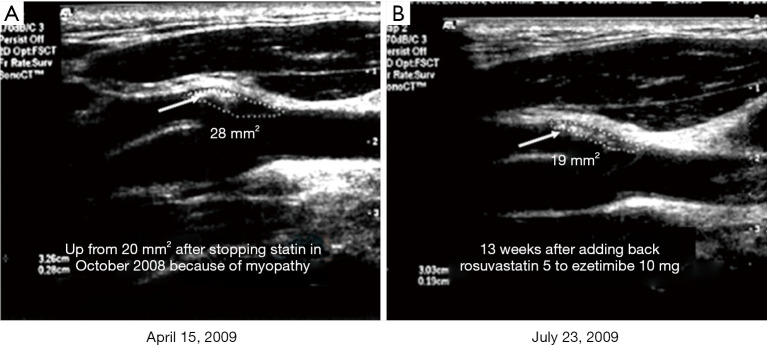
Patients with asymptomatic carotid stenosis (ACS) are at very high risk of coronary events, so they should all receive intensive medical therapy. What is often accepted as "best medical therapy" is usually suboptimal. Truly intensive medical therapy includes lifestyle modification, particularly smoking cessation and a Mediterranean diet. All patients with ACS should receive intensive lipid-lowering therapy, should have their blood pressure well controlled, and should receive B vitamins for lowering of plasma total homocysteine (tHcy) if levels are high; a commonly missed cause of elevated tHcy is metabolic B12 deficiency, which should be diagnosed and treated. Most patients with ACS would be better treated with intensive medical therapy than with either carotid endarterectomy (CEA) or stenting (CAS). A process called "treating arteries instead of treating risk factors" markedly reduced the risk of ACS in an observational study; a randomized trial usual care should be carried out. The few patients with ACS who could benefit (15%, or perhaps more if recent evidence regarding the risk of intraplaque hemorrhage is borne out) can be identified by a number of features. These include microemboli on transcranial Doppler, intraplaque hemorrhage, reduced cerebrovascular reserve, and echolucency of plaques, particularly "juxtaluminal black plaque". No patient should be subjected to CAS or CEA without evidence of high-risk features, because in most cases the 1-year risk of stroke or death with intervention is higher with either CEA (2%) or CAS (4%) than with intensive medical therapy (0.5%). Most patients, particularly the elderly, would be better treated with CEA than CAS. Most strokes can be prevented in patients with ACS, but truly intensive medical therapy is required.
无症状性颈动脉狭窄(ACS)患者发生冠状动脉事件的风险非常高,因此他们都应接受强化药物治疗。通常被认为是“最佳药物治疗”的方案往往并不理想。真正的强化药物治疗包括生活方式的改变,尤其是戒烟和采用地中海饮食。所有ACS患者都应接受强化降脂治疗,血压应得到良好控制,如果血浆总同型半胱氨酸(tHcy)水平升高,应补充B族维生素以降低tHcy水平;tHcy升高常见的一个被漏诊原因是代谢性维生素B12缺乏,应予以诊断和治疗。大多数ACS患者接受强化药物治疗比接受颈动脉内膜切除术(CEA)或支架置入术(CAS)效果更好。在一项观察性研究中,一种被称为“治疗动脉而非治疗危险因素”的方法显著降低了ACS的风险;应开展一项随机试验对比常规治疗。少数能从治疗中获益的ACS患者(约15%,如果关于斑块内出血风险的最新证据得到证实,获益比例可能更高)可通过一些特征来识别。这些特征包括经颅多普勒检测到的微栓子、斑块内出血、脑血管储备降低以及斑块的低回声,尤其是“管腔旁黑色斑块”。没有高危特征证据的患者不应接受CAS或CEA治疗,因为在大多数情况下,CEA(约2%)或CAS(约4%)干预后1年的卒中或死亡风险高于强化药物治疗(约0.5%)。大多数患者,尤其是老年患者,接受CEA治疗比CAS治疗效果更好。ACS患者的大多数卒中是可以预防的,但需要真正的强化药物治疗。