Liverpool School of Tropical Medicine, Liverpool, United Kingdom.
Malawi Liverpool Wellcome Trust Programme, Blantyre, Malawi.
PLoS One. 2020 Nov 12;15(11):e0242226. doi: 10.1371/journal.pone.0242226. eCollection 2020.
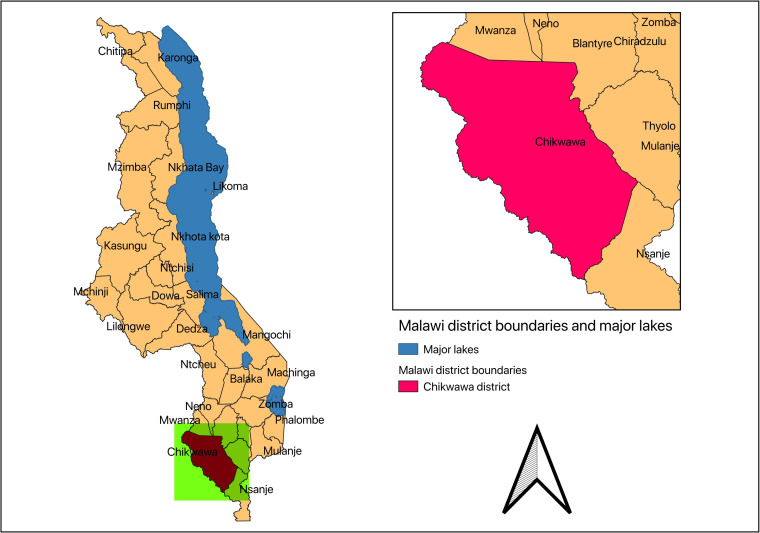
The aim of this article is to provide a detailed description of the Chikwawa lung health cohort which was established in rural Malawi to prospectively determine the prevalence and causes of lung disease amongst the general population of adults living in a low-income rural setting in Sub-Saharan Africa.
A total of 1481 participants were randomly identified and recruited in 2014 for the baseline study. We collected data on demographic, socio-economic status, respiratory symptoms and potentially relevant exposures such as smoking, household fuels, environmental exposures, occupational history/exposures, dietary intake, healthcare utilization, cost (medication, outpatient visits and inpatient admissions) and productivity losses. Spirometry was performed to assess lung function. At baseline, 56.9% of the participants were female, mean age was 43.8 (SD:17.8) and mean body mass index (BMI) was 21.6 Kg/m2 (SD: 3.46).
The cohort has reported the prevalence of chronic respiratory symptoms (13.6%, 95% confidence interval [CI], 11.9-15.4), spirometric obstruction (8.7%, 95% CI, 7.0-10.7), and spirometric restriction (34.8%, 95% CI, 31.7-38.0). Additionally, an annual decline in forced expiratory volume in one second [FEV1] of 30.9mL/year (95% CI: 21.6 to 40.1) and forced vital capacity [FVC] by 38.3 mL/year (95% CI: 28.5 to 48.1) has been reported.
The ongoing phases of follow-up will determine the annual rate of decline in lung function as measured through spirometry and the development of airflow obstruction and restriction, and relate these to morbidity, mortality and economic cost of airflow obstruction and restriction. Population-based mathematical models will be developed driven by the empirical data from the cohort and national population data for Malawi to assess the effects of interventions and programmes to address the lung burden in Malawi. The present follow-up study started in 2019.
本文旨在详细描述奇克瓦瓦肺部健康队列,该队列在马拉维农村建立,旨在前瞻性地确定撒哈拉以南非洲低收入农村环境中成年人的肺部疾病的患病率和病因。
2014 年,共有 1481 名参与者被随机确定并招募参加基线研究。我们收集了人口统计学、社会经济地位、呼吸症状以及潜在相关暴露(如吸烟、家庭燃料、环境暴露、职业史/暴露、饮食摄入、医疗保健利用、成本(药物、门诊就诊和住院)和生产力损失)的数据。进行了肺量测定以评估肺功能。在基线时,56.9%的参与者为女性,平均年龄为 43.8(SD:17.8),平均体重指数(BMI)为 21.6kg/m2(SD:3.46)。
该队列报告了慢性呼吸道症状(13.6%,95%置信区间[CI],11.9-15.4)、肺功能阻塞(8.7%,95%CI,7.0-10.7)和肺功能受限(34.8%,95%CI,31.7-38.0)的患病率。此外,每年第一秒用力呼气量[FEV1]下降 30.9mL/年(95%CI:21.6-40.1)和用力肺活量[FVC]下降 38.3mL/年(95%CI:28.5-48.1)。
正在进行的随访阶段将确定通过肺量测定测量的肺功能每年下降率,以及气流阻塞和限制的发展,并将其与发病率、死亡率以及气流阻塞和限制的经济成本相关联。将由队列的经验数据和马拉维全国人口数据驱动的基于人群的数学模型将被开发出来,以评估解决马拉维肺部负担的干预措施和方案的效果。目前的随访研究于 2019 年开始。