Rheumatology Department, Parc Taulí University Hospital, I3PT Research Institute (UAB), Universitat Autónoma de Barcelona (UAB), 08208 Sabadell, Spain.
Immunology Unit UDIAT, Parc Taulí University Hospital. I3PT Research Institute (UAB), 08208 Sabadell, Spain.
Viruses. 2020 Nov 9;12(11):1277. doi: 10.3390/v12111277.
COVID-19 pathophysiology and the predictive factors involved are not fully understood, but lymphocytes dysregulation appears to play a role. This paper aims to evaluate lymphocyte subsets in the pathophysiology of COVID-19 and as predictive factors for severe disease.
A prospective cohort study of patients with SARS-CoV-2 bilateral pneumonia recruited at hospital admission. Demographics, medical history, and data regarding SARS-CoV-2 infection were recorded. Patients systematically underwent complete laboratory tests, including parameters related to COVID-19 as well as lymphocyte subsets study at the time of admission. Severe disease criteria were established at admission, and patients were classified on remote follow-up according to disease evolution. Linear regression models were used to assess associations with disease evolution, and Receiver Operating Characteristic (ROC) and the corresponding Area Under the Curve (AUC) were used to evaluate predictive values.
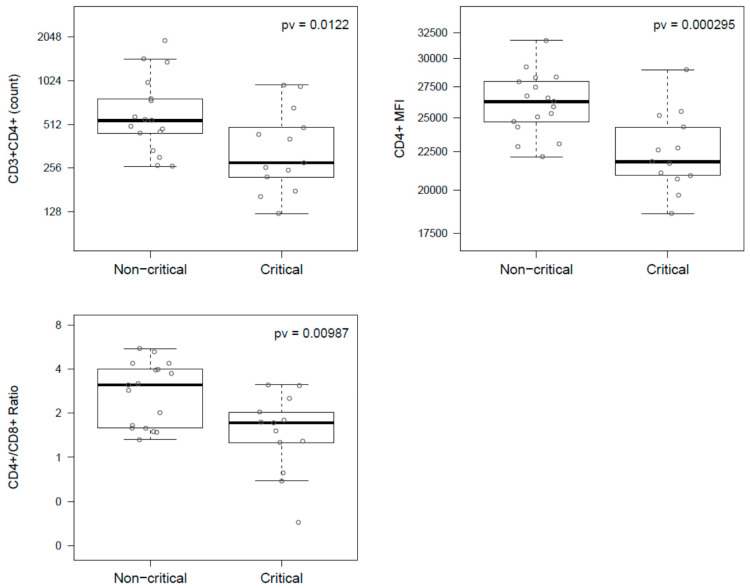
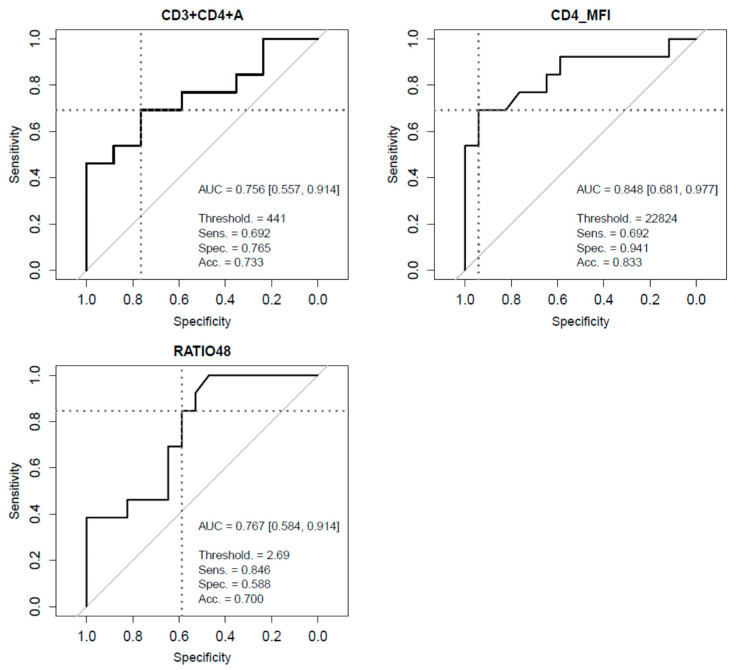
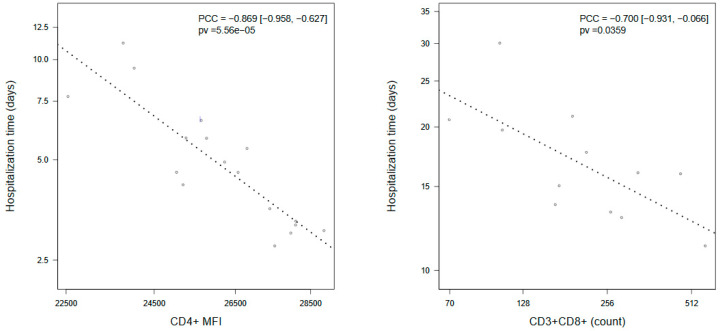
Patients with critical COVID-19 showed a decrease in CD3+CD4+ T cells count compared to non-critical (278 (485 IQR) vs. 545 (322 IQR)), a decrease in median CD4+/CD8+ ratio (1.7, (1.7 IQR) vs. 3.1 (2.4 IQR)), and a decrease in median CD4+MFI (21,820 (4491 IQR) vs. 26,259 (3256 IQR)), which persisted after adjustment. CD3+CD8+ T cells count had a high correlation with time to hospital discharge (PC = -0.700 (-0.931, -0.066)). ROC curves for predictive value showed lymphocyte subsets achieving the best performances, specifically CD3+CD4+ T cells (AUC = 0.756), CD4+/CD8+ ratio (AUC = 0.767), and CD4+MFI (AUC = 0.848).
A predictive value and treatment considerations for lymphocyte subsets are suggested, especially for CD3CD4+ T cells. Lymphocyte subsets determination at hospital admission is recommended.
COVID-19 的病理生理学和涉及的预测因素尚未完全了解,但淋巴细胞失调似乎发挥了作用。本文旨在评估 COVID-19 病理生理学中的淋巴细胞亚群,并将其作为疾病严重程度的预测因素。
对在入院时患有 SARS-CoV-2 双侧肺炎的患者进行了一项前瞻性队列研究。记录了人口统计学、病史和 SARS-CoV-2 感染数据。患者系统地接受了完整的实验室检查,包括与 COVID-19 相关的参数以及入院时的淋巴细胞亚群研究。在入院时确定了严重疾病的标准,并根据疾病的演变在远程随访时对患者进行分类。使用线性回归模型评估与疾病演变的关联,并使用接收器工作特征(ROC)和相应的曲线下面积(AUC)评估预测值。
与非重症 COVID-19 患者相比,重症 COVID-19 患者的 CD3+CD4+T 细胞计数减少(278(485 IQR)比 545(322 IQR)),CD4+/CD8+比值中位数降低(1.7(1.7 IQR)比 3.1(2.4 IQR)),CD4+MFI 中位数降低(21,820(4491 IQR)比 26,259(3256 IQR)),调整后仍持续存在。CD3+CD8+T 细胞计数与住院时间呈高度相关(PC = -0.700(-0.931,-0.066))。预测值的 ROC 曲线显示,淋巴细胞亚群表现出最佳性能,特别是 CD3+CD4+T 细胞(AUC = 0.756)、CD4+/CD8+比值(AUC = 0.767)和 CD4+MFI(AUC = 0.848)。
建议对淋巴细胞亚群进行预测价值和治疗考虑,特别是对 CD3+CD4+T 细胞。建议在入院时测定淋巴细胞亚群。