Sirico Marianna, Bernocchi Ottavia, Sobhani Navid, Giudici Fabiola, Corona Silvia P, Vernieri Claudio, Nichetti Federico, Cappelletti Maria Rosa, Milani Manuela, Strina Carla, Cervoni Valeria, Barbieri Giuseppina, Ziglioli Nicoletta, Dester Martina, Bianchi Giulia Valeria, De Braud Filippo, Generali Daniele
Department of Surgery and Cancer, Imperial College London, London W12 0NN, UK.
Azienda Socio-Sanitaria Territoriale Cremona, 26100 Cremona, Italy.
Cancers (Basel). 2020 Nov 10;12(11):3314. doi: 10.3390/cancers12113314.
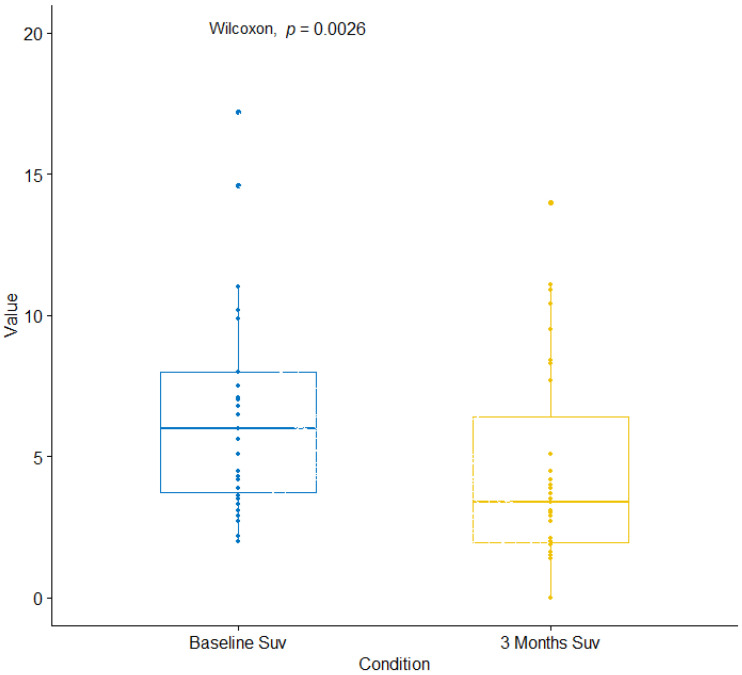
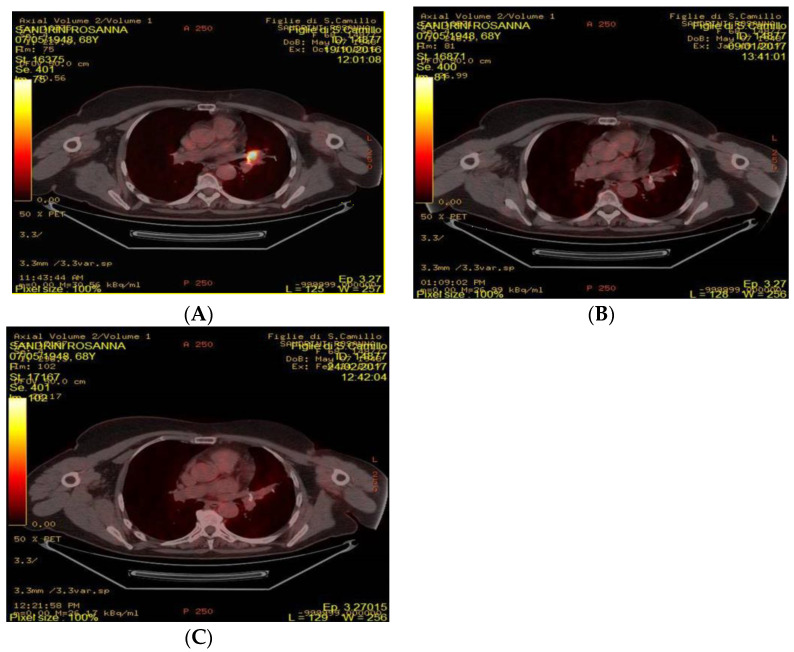
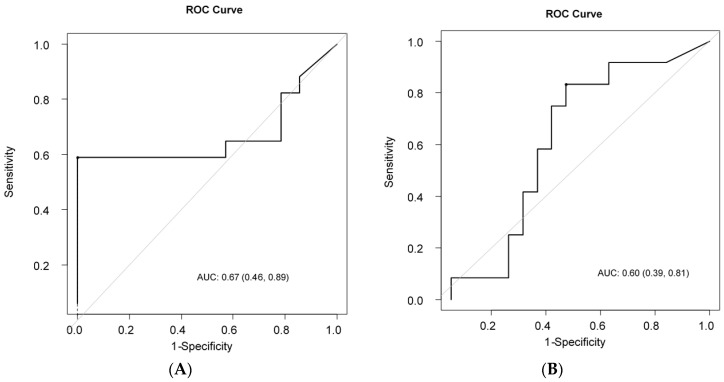
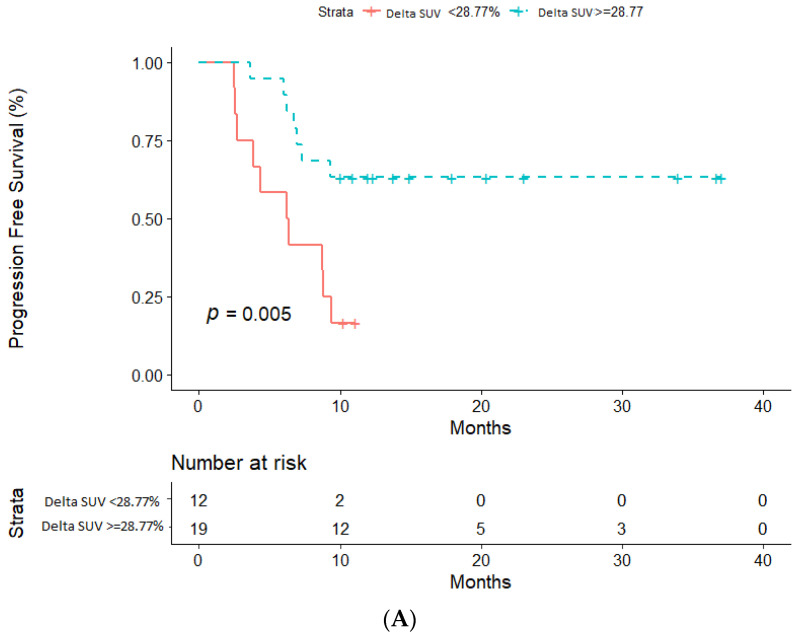
The mTORC1 inhibitor everolimus has been approved in combination with the aromatase inhibitor exemestane for the treatment of hormone receptor-positive (HR+) human epidermal growth factor receptor 2-negative (HER2-) metastatic breast cancer (HR+ mBC) progressing on prior therapy with a non-steroidal aromatase inhibitor. To date, no predictive biomarkers of tumor sensitivity/resistance for everolimus-based treatments have been identified. We hypothesized that precocious changes in the Standardized Uptake Volume (∆SUV%), as assessed by F-Fluorodeoxyglucosepositron-emission tomography (F-FDG PET/CT), may be a marker of everolimus efficacy. This was a retrospective study including 31 HR+ HER2- patients treated with everolimus and exemestane in two Italian centers between 2013 and 2018. The objective of the study was to investigate ∆SUV% as a predictive marker of everolimus antitumor efficacy. F-FDG PET/CT scans were performed at baseline and after three months of treatment. Patients were defined as long responders (LRs) if disease progression occurred at least 10 months after treatment initiation and long survivors (LSs) if death occurred later than 36 months after starting therapy. ROC analysis was used to determine the optimal cut-off values of ∆SUV% to distinguish LRs from non-LRs and LSs from non-LSs. Progression-free survival (PFS) and overall survival (OS) were estimated by Kaplan-Meier method. The SUVmax values decreased significantly from baseline to 3 months after therapy ( = 0.003). Dynamic changes of SUVmax (Delta SUV) had a higher accuracy in discriminating long-responders from non-long-responders (AUC = 0.67, Delta SUV cut-off = 28.8%) respects to its ability to identify long survivors from no-long survivors (AUC = 0.60, Delta SUV cut-off = 53.8%). Patients were divided into groups according to the Delta SUV cut-offs and survival outcomes were evaluated: patients with a decrease of ∆SUV% ≥ 28.8% had significantly better PFS (10 months-PFS: 63.2%, 95% CI: 37.9-80.4% and 16.7%, 95% CI: 2.7-41.3% respectively, = 0.005). As regard as OS, patients with ∆SUV% ≥ 53.8% had longer OS when compared to patients with ∆SUV% < 53.8% (36 month-OS: 82.5% vs. 45.9% vs. = 0.048). We found two precocious ∆SUV% thresholds capable of identifying HR+ HER2-mBC patients, which would achieve long-term benefit or long-term survival during everolimus-exemestane therapy. These results warrant further validation in prospective studies and should be integrated with molecular biomarkers related to tumor metabolism and mTORC1 signaling.
mTORC1抑制剂依维莫司已被批准与芳香化酶抑制剂依西美坦联合使用,用于治疗激素受体阳性(HR+)、人表皮生长因子受体2阴性(HER2-)的转移性乳腺癌(HR+ mBC),这些患者在接受非甾体芳香化酶抑制剂的先前治疗后病情进展。迄今为止,尚未发现基于依维莫司治疗的肿瘤敏感性/耐药性预测生物标志物。我们假设,通过F-氟脱氧葡萄糖正电子发射断层扫描(F-FDG PET/CT)评估的标准化摄取值(∆SUV%)的早熟变化可能是依维莫司疗效的标志物。这是一项回顾性研究,纳入了2013年至2018年期间在两个意大利中心接受依维莫司和依西美坦治疗的31例HR+ HER2-患者。该研究的目的是调查∆SUV%作为依维莫司抗肿瘤疗效的预测标志物。在基线和治疗三个月后进行F-FDG PET/CT扫描。如果疾病进展发生在治疗开始后至少10个月,则将患者定义为长期缓解者(LRs);如果死亡发生在开始治疗后36个月之后,则将患者定义为长期存活者(LSs)。采用ROC分析确定∆SUV%的最佳临界值,以区分LRs与非LRs以及LSs与非LSs。采用Kaplan-Meier法估计无进展生存期(PFS)和总生存期(OS)。治疗后3个月时SUVmax值较基线显著降低(P = 0.003)。SUVmax的动态变化(Delta SUV)在区分长期缓解者与非长期缓解者方面具有更高的准确性(AUC = 0.67,Delta SUV临界值 = 28.8%),而在识别长期存活者与非长期存活者方面的能力相对较低(AUC = 0.60,Delta SUV临界值 = 53.8%)。根据Delta SUV临界值将患者分组并评估生存结果:∆SUV%下降≥28.8%的患者PFS显著更好(10个月PFS:分别为63.2%,95% CI:37.9 - 80.4%和16.7%,95% CI:2.7 - 41.3%,P = 0.005)。关于OS,∆SUV%≥53.8%的患者与∆SUV%<53.8%的患者相比,OS更长(36个月OS:82.5%对45.9%,P = 0.048)。我们发现了两个早熟的∆SUV%临界值,能够识别HR+ HER2- mBC患者,这些患者在依维莫司 - 依西美坦治疗期间将实现长期获益或长期存活。这些结果有待在前瞻性研究中进一步验证,并应与与肿瘤代谢和mTORC1信号传导相关的分子生物标志物相结合。