Frankland Jane, Wheelwright Sally, Permyakova Natalia V, Wright David, Collaço Nicole, Calman Lynn, Winter Jane, Fenlon Deborah, Richardson Alison, Smith Peter W, Foster Claire
Macmillan Survivorship Research Group, School of Health Sciences, University of Southampton, Southampton, UK.
University Hospital Southampton NHS Foundation Trust, Southampton, UK.
BMJ Open. 2020 Nov 12;10(11):e038953. doi: 10.1136/bmjopen-2020-038953.
To describe prevalence and predictors of poor sexual well-being for men and women over 5 years following treatment for colorectal cancer.
Prospective longitudinal study, from presurgery to 5 years postsurgery, with eight assessment points. Logistic regression models predicted sexual well-being from presurgery to 24 months and 24 months to 60 months; time-adjusted then fully adjusted models were constructed at each stage.
Twenty-nine hospitals in the UK.
Patients with Dukes' stage A-C, treated with curative intent, aged ≥18 years and able to complete questionnaires were eligible.
The dependent variable was the Quality of Life in Adult Cancer Survivors sexual function score. Independent variables included sociodemographic, clinical and psychosocial characteristics.
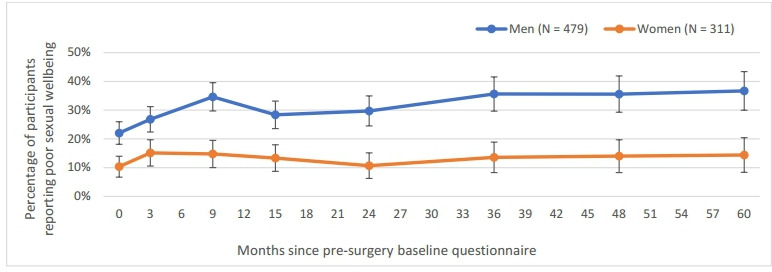
Seven hundred and ninety participants provided a sexual well-being score for at least one time point. Thirty-seven per cent of men and 14% of women reported poor sexual well-being at 5 years. Baseline predictors for men at 24 months included having a stoma (OR 1.5, 95% CI 1.02 to 2.20) and high levels of depression (OR 2.69/2.01, 95% CI 1.68 to 4.32/1.12 to 3.61); men with high self-efficacy (OR confident 0.33/0.48, 95% CI 0.18 to 0.61/0.24 to 1.00; very confident 0.25/0.42, 95% CI 0.13 to 0.49/0.19 to 0.94) and social support (OR 0.52/0.56, 95% CI 0.33 to 0.81/0.35 to 0.91) were less likely to report poor sexual well-being. Predictors at 60 months included having a stoma (OR 2.30/2.67, 95% CI 1.22 to 4.34/1.11 to 6.40) and high levels of depression (OR 5.61/2.58, 95% CI 2.58 to 12.21/0.81 to 8.25); men with high self-efficacy (very confident 0.14, 95% CI 0.047 to 0.44), full social support (OR 0.26; 95% CI 0.13 to 0.53) and higher quality of life (OR 0.97, 95% CI 0.95 to 0.98) were less likely to report poor sexual well-being. It was not possible to construct models for women due to low numbers reporting poor sexual well-being.
Several psychosocial variables were identified as predictors of poor sexual well-being among men. Interventions targeting low self-efficacy may be helpful. More research is needed to understand women's sexual well-being.
描述结直肠癌治疗后5年男性和女性性功能不良的患病率及预测因素。
前瞻性纵向研究,从术前到术后5年,共8个评估点。逻辑回归模型预测术前至术后24个月以及术后24个月至60个月的性功能状况;在每个阶段构建时间调整模型,然后进行完全调整模型。
英国29家医院。
符合条件的患者为年龄≥18岁、接受根治性治疗、处于Dukes A - C期且能够完成问卷的患者。
因变量为成年癌症幸存者性功能评分中的生活质量。自变量包括社会人口学、临床和心理社会特征。
790名参与者至少在一个时间点提供了性功能评分。5年时,37%的男性和14%的女性报告性功能不良。术后24个月男性的基线预测因素包括造口(比值比1.5,95%置信区间1.02至2.20)和高抑郁水平(比值比2.69/2.01,95%置信区间1.68至4.32/1.12至3.61);自我效能感高的男性(自信:比值比0.33/0.48,95%置信区间0.18至0.61/0.24至1.00;非常自信:比值比0.25/0.42,95%置信区间0.13至0.49/0.19至0.94)和社会支持高的男性(比值比0.52/0.56,95%置信区间0.33至0.81/0.35至0.91)报告性功能不良的可能性较小。术后60个月的预测因素包括造口(比值比2.30/2.67,95%置信区间1.22至4.34/1.11至6.40)和高抑郁水平(比值比5.61/2.58,95%置信区间2.58至12.21/0.81至8.25);自我效能感高(非常自信:比值比0.14,95%置信区间0.047至0.44)、完全社会支持(比值比0.26;95%置信区间0.13至0.53)和生活质量较高(比值比0.97,95%置信区间0.95至0.98)的男性报告性功能不良的可能性较小。由于报告性功能不良的女性数量较少,无法为女性构建模型。
确定了几个心理社会变量为男性性功能不良的预测因素。针对低自我效能感的干预可能会有帮助。需要更多研究来了解女性的性功能状况。