Department of Medicine Solna, Clinical Epidemiology Division, Karolinska Institutet, Stockholm, Sweden.
Department of Medical Epidemiology and Biostatistics, Karolinska Institutet, Stockholm, Sweden.
Transfusion. 2021 Feb;61(2):464-473. doi: 10.1111/trf.16175. Epub 2020 Nov 13.
Recently, plateletpheresis donations using a widely used leukoreduction system (LRS) chamber have been associated with T-cell lymphopenia. However, clinical health consequences of plateletpheresis-associated lymphopenia are still unknown.
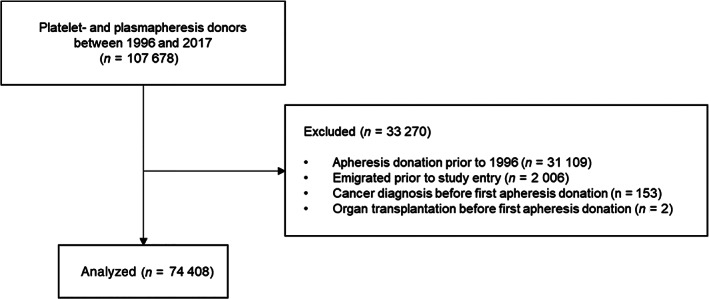
A nationwide cohort study using the SCANDAT3-S database was conducted with all platelet- and plasmapheresis donors in Sweden between 1996 and 2017. A Cox proportional hazards model, using donations as time-dependent exposures, was used to assess the risk of infections associated with plateletpheresis donations using an LRS chamber.
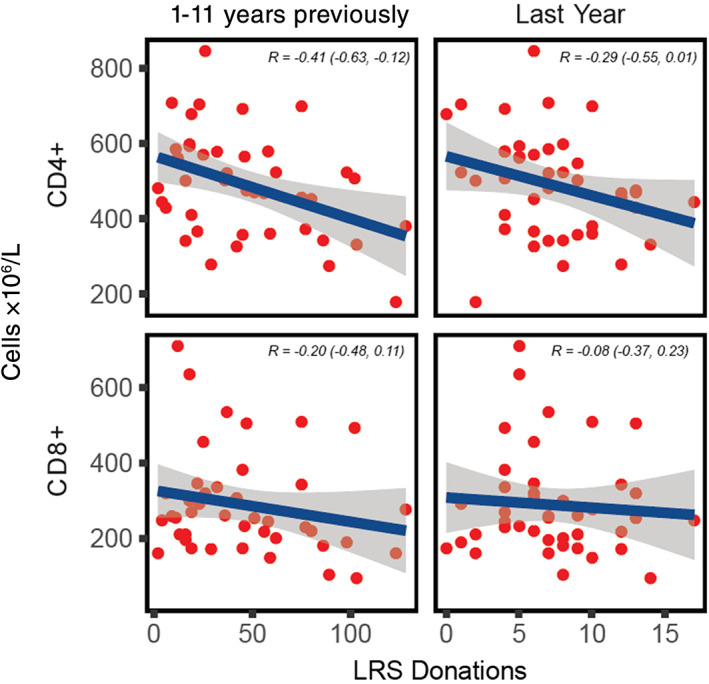
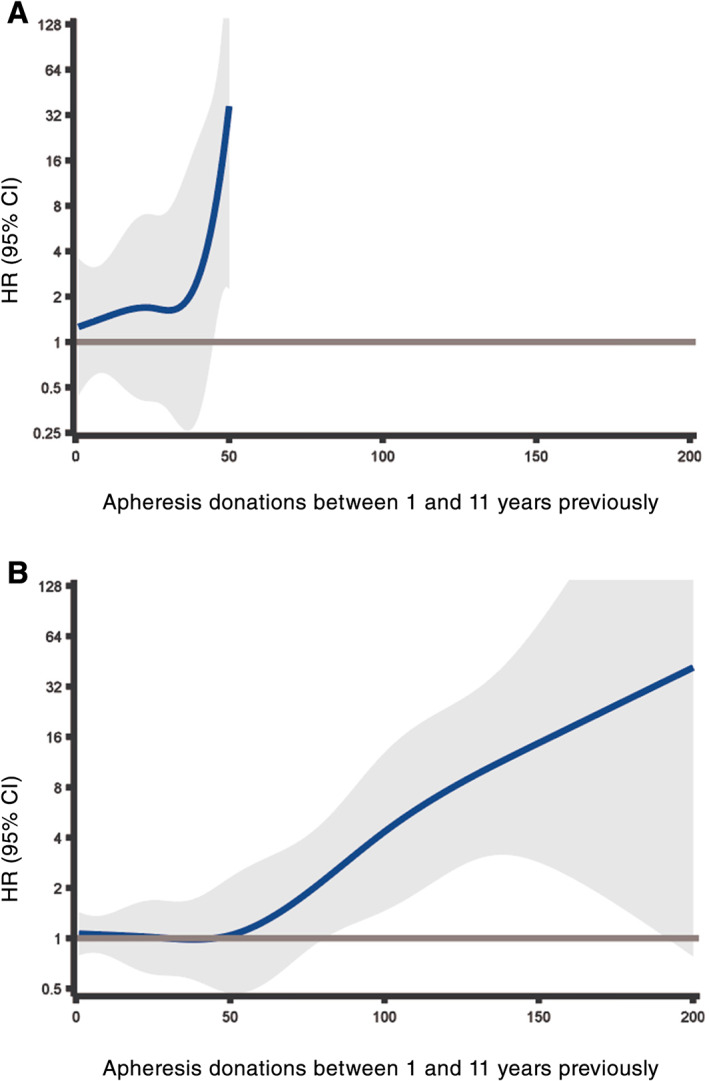
A total of 74 408 apheresis donors were included. Among donors with the same donation frequency, plateletpheresis donors using an LRS chamber were at an increased risk of immunosuppression-related infections and common bacterial infections in a dose-dependent manner. While very frequent donors and infections were rare in absolute terms resulting in wide confidence intervals (CIs), the increased risk was significant starting at one-third or less of the allowed donation frequency in a 10-year exposure window, with hazard ratios reaching 10 or more. No plateletpheresis donors that used an LRS chamber experienced a Pneumocystis jirovecii, aspergillus, disseminated mycobacterial, or cryptococcal infection. In a subcohort (n = 42), donations with LRS were associated with low CD4+ T-cell counts (Pearson's R = -0.41; 95% CI, - 0.63 to -0.12).
Frequent plateletpheresis donation using an LRS chamber was associated with CD4+ T-cell lymphopenia and an increased risk of infections. These findings suggest a need to monitor T-lymphocyte counts in frequent platelet donors and to conduct future investigations of long-term donor health and for regulators to consider steps to mitigate lymphodepletion in donors.
最近,使用广泛使用的白细胞减少系统(LRS)室进行血小板单采术与 T 细胞淋巴细胞减少有关。然而,血小板单采术相关淋巴细胞减少的临床健康后果尚不清楚。
使用瑞典 1996 年至 2017 年间所有血小板和血浆单采术供体的 SCANDAT3-S 数据库进行了一项全国性队列研究。使用 Cox 比例风险模型,以捐赠作为时间依赖性暴露,评估使用 LRS 室进行血小板单采术与感染相关的风险。
共纳入 74408 名单采术供体。在具有相同捐献频率的供体中,使用 LRS 室的血小板单采术供体以剂量依赖性方式增加了与免疫抑制相关的感染和常见细菌感染的风险。虽然非常频繁的供体和感染在绝对值上很少见,导致置信区间(CI)很宽,但在 10 年暴露窗口内允许捐献频率的三分之一或更少开始,风险比达到 10 或更高。没有使用 LRS 室的血小板单采术供体经历过卡氏肺孢子虫、曲霉菌、播散性分枝杆菌或隐球菌感染。在一个亚队列(n = 42)中,LRS 捐赠与 CD4+ T 细胞计数低有关(Pearson's R = -0.41;95%CI,-0.63 至 -0.12)。
频繁使用 LRS 室进行血小板单采术与 CD4+ T 细胞淋巴细胞减少和感染风险增加有关。这些发现表明需要监测频繁的血小板供体中的 T 淋巴细胞计数,并对长期供体健康进行进一步研究,供体监管机构考虑采取措施减轻供体的淋巴细胞减少。