Department of Internal Medicine, Foch Hospital, F-92151, Suresnes, France.
Diagnosis and Therapeutic Center, Hypertension and Cardiovascular Prevention Unit, AP-HP, Hôtel-Dieu Hospital, Paris-Descartes University, Paris, France.
J Clin Immunol. 2021 Feb;41(2):303-314. doi: 10.1007/s10875-020-00911-6. Epub 2020 Nov 14.
High levels of serum interleukin-6 (IL-6) correlate with disease severity in COVID-19. We hypothesized that tocilizumab (a recombinant humanized anti-IL-6 receptor) could improve outcomes in selected patients with severe worsening COVID-19 pneumonia and high inflammatory parameters.
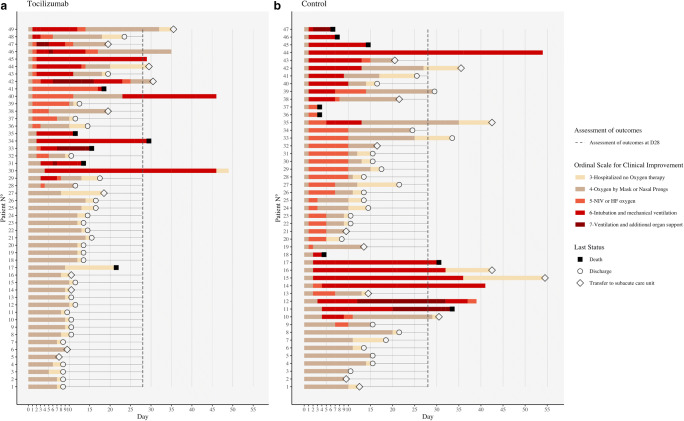
The TOCICOVID study included a prospective cohort of patients aged 16-80 years with severe (requiring > 6 L/min of oxygen therapy to obtain Sp02 > 94%) rapidly deteriorating (increase by ≥ 3 L/min of oxygen flow within the previous 12 h) COVID-19 pneumonia with ≥ 5 days of symptoms and C-reactive protein levels > 40 mg/L. They entered a compassionate use program of treatment with intravenous tocilizumab (8 mg/kg with a maximum of 800 mg per infusion; and if needed a second infusion 24 to 72 h later). A control group was retrospectively selected with the same inclusion criteria. Outcomes were assessed at D28 using inverse probability of treatment weighted (IPTW) methodology.
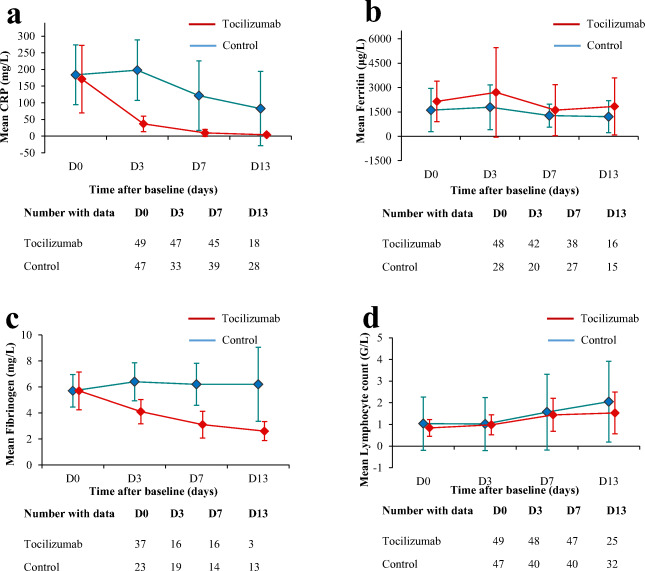
Among the 96 patients included (81% male, mean (SD) age: 60 (12.5) years), underlying conditions, baseline disease severity, and concomitant medications were broadly similar between the tocilizumab (n = 49) and the control (n = 47) groups. In the IPTW analysis, treatment with tocilizumab was associated with a reduced need for overall ventilatory support (49 vs. 89%, wHR: 0.39 [0.25-0.56]; p < 0.001). Albeit lacking statistical significance, there was a substantial trend towards a reduction of mechanical ventilation (31% vs. 45%; wHR: 0.58 [0.36-0.94]; p = 0.026). However, tocilizumab did not improve overall survival (wHR = 0.68 [0.31-1.748], p = 0.338). Among the 85 (89%) patients still alive at D28, patients treated with tocilizumab had a higher rate of oxygen withdrawal (82% vs. 73.5%, wHR = 1.66 [1.17-2.37], p = 0.005), with a shorter delay before being weaned of oxygen therapy (mean 11 vs. 16 days; p < 0.001). At D28, the rate of patients discharged from hospital was higher in the tocilizumab group (70% vs. 40%, wHR = 1.82 [1.22-2.75]; p = 0.003). The levels of CRP and fibrinogen post therapy (p < 0.001 for both variables) were significantly lower in the tocilizumab group (interaction test, mixed model). Rates of neutropenia (35% vs. 0%; p < 0.001) were higher in the tocilizumab group, yet rates of infections (22% vs. 38%, p = 0.089) including ventilator-acquired pneumonia (8% vs. 26%, p = 0.022) were higher in the control group.
These data could be helpful for the design of future trials aiming to counter COVID-19-induced inflammation, especially before patients require admission to the intensive care unit.
血清白细胞介素-6(IL-6)水平高与 COVID-19 患者的疾病严重程度相关。我们假设托珠单抗(一种重组人源化抗 IL-6 受体)可以改善选择的重症 COVID-19 肺炎和高炎症参数患者的预后。
TOCICOVID 研究纳入了年龄在 16-80 岁之间的前瞻性队列患者,这些患者患有严重(需要 >6L/min 的氧气治疗才能使 Sp02>94%)快速恶化(在过去 12 小时内增加 >3L/min 的氧气流量)的 COVID-19 肺炎,且症状持续时间≥5 天,C 反应蛋白水平 >40mg/L。他们进入了托珠单抗静脉注射的同情使用计划(8mg/kg,最大剂量为 800mg/次输注;如果需要,24 至 72 小时后进行第二次输注)。对照组是根据相同的纳入标准通过回顾性选择的。使用逆概率治疗加权(IPTW)方法在 D28 评估结局。
在纳入的 96 名患者(81%为男性,平均(SD)年龄:60(12.5)岁)中,托珠单抗组(n=49)和对照组(n=47)的基础疾病、基线疾病严重程度和伴随药物使用情况广泛相似。在 IPTW 分析中,托珠单抗治疗与总体通气支持需求降低相关(49% vs. 89%,加权风险比:0.39[0.25-0.56];p<0.001)。虽然缺乏统计学意义,但机械通气的使用有显著减少的趋势(31% vs. 45%;加权风险比:0.58[0.36-0.94];p=0.026)。然而,托珠单抗并不能改善总体生存率(加权风险比:0.68[0.31-1.748],p=0.338)。在 D28 仍存活的 85 名(89%)患者中,接受托珠单抗治疗的患者吸氧撤机率更高(82% vs. 73.5%,加权风险比:1.66[1.17-2.37],p=0.005),氧疗脱机前的延迟时间更短(平均 11 天 vs. 16 天;p<0.001)。在 D28,托珠单抗组的出院率更高(70% vs. 40%,加权风险比:1.82[1.22-2.75];p=0.003)。治疗后 CRP 和纤维蛋白原水平(均为 p<0.001)在托珠单抗组显著降低(交互检验,混合模型)。托珠单抗组中性粒细胞减少症发生率(35% vs. 0%;p<0.001)更高,但对照组的感染发生率(22% vs. 38%,p=0.089)包括呼吸机相关性肺炎(8% vs. 26%,p=0.022)更高。
这些数据可能有助于设计针对 COVID-19 诱导的炎症的未来试验,特别是在患者需要入住重症监护病房之前。