De Luca Giacomo, Cavalli Giulio, Campochiaro Corrado, Della-Torre Emanuel, Angelillo Piera, Tomelleri Alessandro, Boffini Nicola, Tentori Stefano, Mette Francesca, Farina Nicola, Rovere-Querini Patrizia, Ruggeri Annalisa, D'Aliberti Teresa, Scarpellini Paolo, Landoni Giovanni, De Cobelli Francesco, Paolini John F, Zangrillo Alberto, Tresoldi Moreno, Trapnell Bruce C, Ciceri Fabio, Dagna Lorenzo
Unit of Immunology, Rheumatology, Allergy and Rare Diseases, IRCCS San Raffaele Scientific Institute, Milan, Italy.
Vita-Salute San Raffaele University, Milan, Italy.
Lancet Rheumatol. 2020 Aug;2(8):e465-e473. doi: 10.1016/S2665-9913(20)30170-3. Epub 2020 Jun 16.
Mortality in patients with COVID-19 pneumonia and systemic hyperinflammation is high. We aimed to examine whether mavrilimumab, an anti-granulocyte-macrophage colony-stimulating factor receptor-α monoclonal antibody, added to standard management, improves clinical outcomes in patients with COVID-19 pneumonia and systemic hyperinflammation.
This single-centre prospective cohort study included patients aged 18 years or older who were admitted to San Raffaele Hospital (Milan, Italy) with severe COVID-19 pneumonia, hypoxia, and systemic hyperinflammation. Patients received a single intravenous dose (6 mg/kg) of mavrilimumab added to standard care given by the hospital at the time. The control group consisted of contemporaneous patients with similar baseline characteristics who received standard care at the same hospital. The main outcome was time to clinical improvement (defined as improvement of two or more points on the seven-point ordinal scale of clinical status). Other outcomes included proportion of patients achieving clinical improvement, survival, mechanical ventilation-free survival, and time to fever resolution. Adverse events were monitored daily.
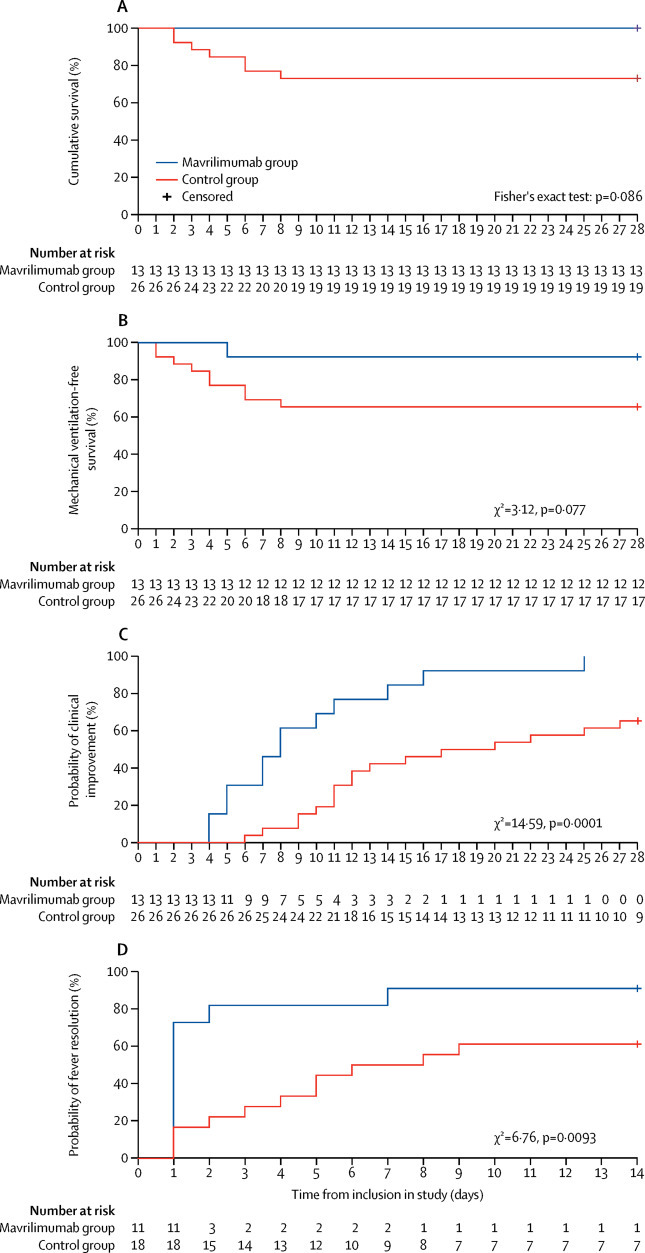
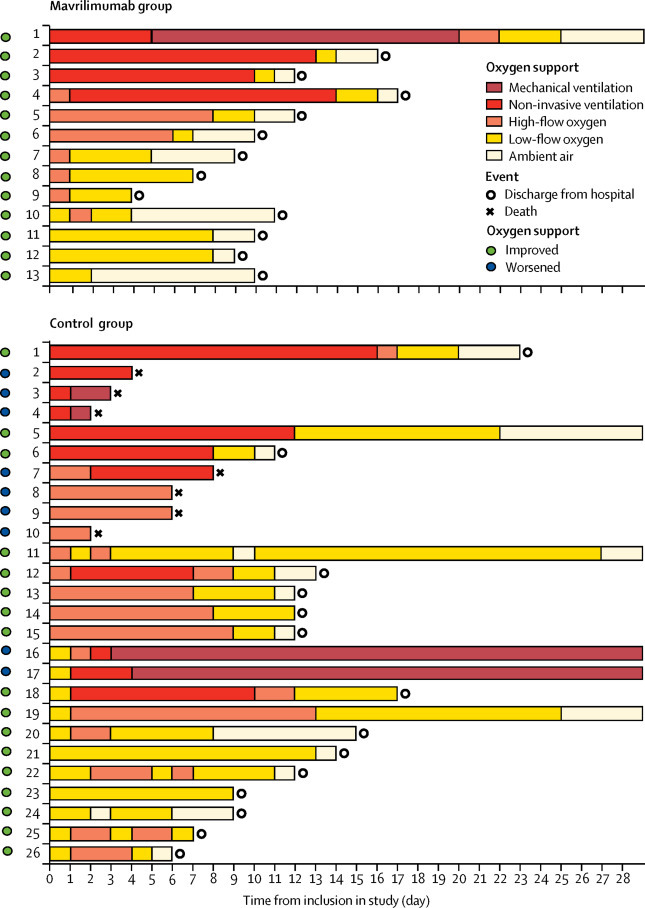
Between March 17 and April 15, 2020, 13 non-mechanically ventilated patients (median age 57 years [IQR 52-58], 12 [92%] men) received mavrilimumab and 26 patients (median age 60 [IQR 53-67], 17 [65%] men) in the control group received standard care. During the 28-day follow-up, no patients in the mavrilimumab group died, and seven (27%) patients in the control group died (p=0·086). At day 28, all patients in the mavrilimumab group and 17 (65%) patients in the control group showed clinical improvement (p=0·030), with earlier improvement in the mavrilimumab than in the control group (mean time to improvement 8 days [IQR 5 to 11] 19 days [11 to >28], p=0·0001). By day 28, one (8%) patient in the mavrilimumab group progressed to mechanical ventilation compared with nine (35%) patients in the control group who progressed to mechanical ventilation or died (p=0·14). By day 14, fever resolved in ten (91%) of 11 febrile patients in the mavrilimumab group, compared with 11 (61%) of 18 febrile patients in the control group (p=0·18); fever resolution was faster in mavrilimumab recipients versus controls (median time to resolution 1 day [IQR 1 to 2] 7 days [3 to >14], p=0·0093). Mavrilimumab was well tolerated, with no infusion reactions. Three (12%) patients in the control group developed infectious complications.
Mavrilimumab treatment was associated with improved clinical outcomes compared with standard care in non-mechanically ventilated patients with severe COVID-19 pneumonia and systemic hyperinflammation. Treatment was well tolerated. Confirmation of efficacy requires controlled testing.
IRCCS San Raffaele Scientific Institute.
新型冠状病毒肺炎(COVID-19)合并全身炎症反应患者的死亡率很高。我们旨在研究在标准治疗基础上加用抗粒细胞-巨噬细胞集落刺激因子受体-α单克隆抗体mavrilimumab是否能改善COVID-19肺炎合并全身炎症反应患者的临床结局。
这项单中心前瞻性队列研究纳入了年龄在18岁及以上、因严重COVID-19肺炎、低氧血症和全身炎症反应入住意大利米兰圣拉斐尔医院的患者。患者在接受医院当时给予的标准治疗的基础上,静脉注射单剂量(6mg/kg)的mavrilimumab。对照组由同期在同一家医院接受标准治疗、基线特征相似的患者组成。主要结局是临床改善时间(定义为临床状态七点序贯量表上提高两分或更多)。其他结局包括实现临床改善的患者比例、生存率、无机械通气生存率以及发热消退时间。每天监测不良事件。
2020年3月17日至4月15日,13例非机械通气患者(中位年龄57岁[四分位间距52 - 58],12例[92%]为男性)接受了mavrilimumab治疗,对照组26例患者(中位年龄60岁[四分位间距53 - 67],17例[65%]为男性)接受了标准治疗。在28天的随访期间,mavrilimumab组无患者死亡,对照组有7例(27%)患者死亡(p = 0.086)。在第28天时,mavrilimumab组所有患者和对照组17例(65%)患者显示临床改善(p = 0.030),mavrilimumab组的改善早于对照组(平均改善时间8天[四分位间距5至11]对19天[11至>28],p = 0.0001)。到第28天时,mavrilimumab组1例(8%)患者进展为机械通气,而对照组9例(35%)患者进展为机械通气或死亡(p = 0.14)。到第14天时,mavrilimumab组11例发热患者中有10例(91%)发热消退,而对照组18例发热患者中有11例(61%)发热消退(p = 0.18);mavrilimumab治疗组患者发热消退比对照组更快(中位消退时间1天[四分位间距1至2]对7天[3至>14],p = 0.0093)。mavrilimumab耐受性良好,无输液反应。对照组3例(12%)患者出现感染性并发症。
与标准治疗相比,mavrilimumab治疗可改善非机械通气的重症COVID-19肺炎合并全身炎症反应患者的临床结局。该治疗耐受性良好。疗效的确证需要对照试验。
IRCCS圣拉斐尔科学研究所。