Posti Jussi P, Takala Riikka S K, Raj Rahul, Luoto Teemu M, Azurmendi Leire, Lagerstedt Linnéa, Mohammadian Mehrbod, Hossain Iftakher, Gill Jessica, Frantzén Janek, van Gils Mark, Hutchinson Peter J, Katila Ari J, Koivikko Pia, Maanpää Henna-Riikka, Menon David K, Newcombe Virginia F, Tallus Jussi, Blennow Kaj, Tenovuo Olli, Zetterberg Henrik, Sanchez Jean-Charles
Clinical Neurosciences, Department of Neurosurgery, Turku Brain Injury Centre, Turku University Hospital, University of Turku, Turku, Finland.
Perioperative Services, Intensive Care Medicine and Pain Management, Department of Anesthesiology and Intensive Care, Turku University Hospital, University of Turku, Turku, Finland.
Front Neurol. 2020 Oct 30;11:549527. doi: 10.3389/fneur.2020.549527. eCollection 2020.
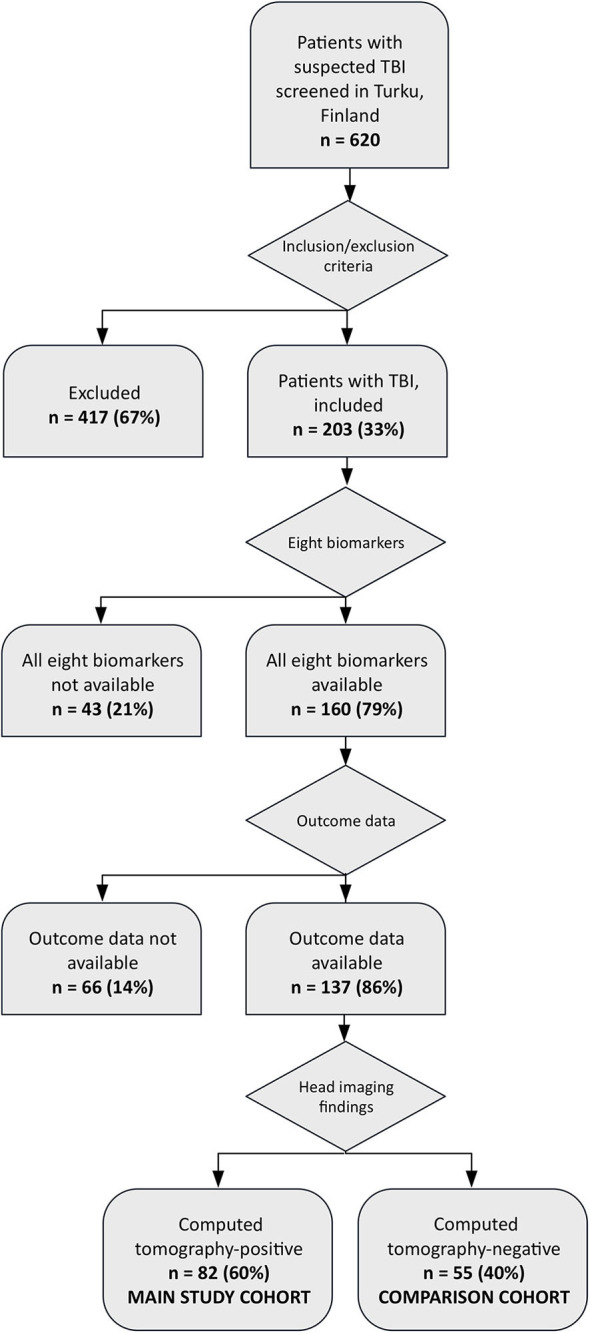
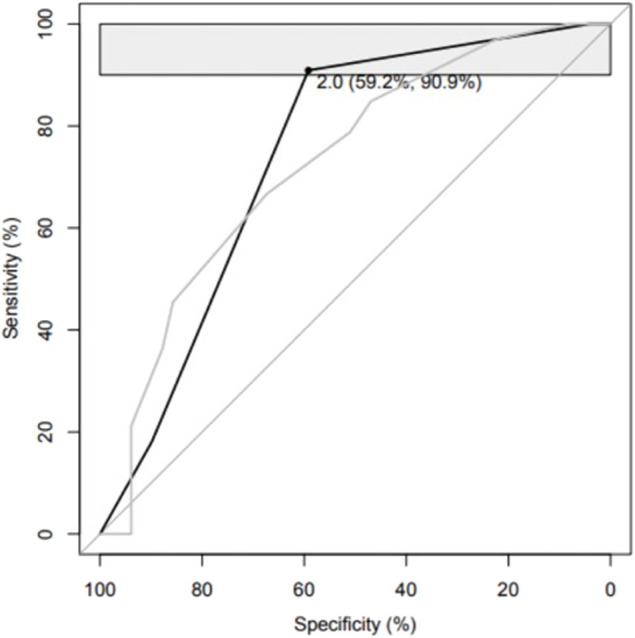
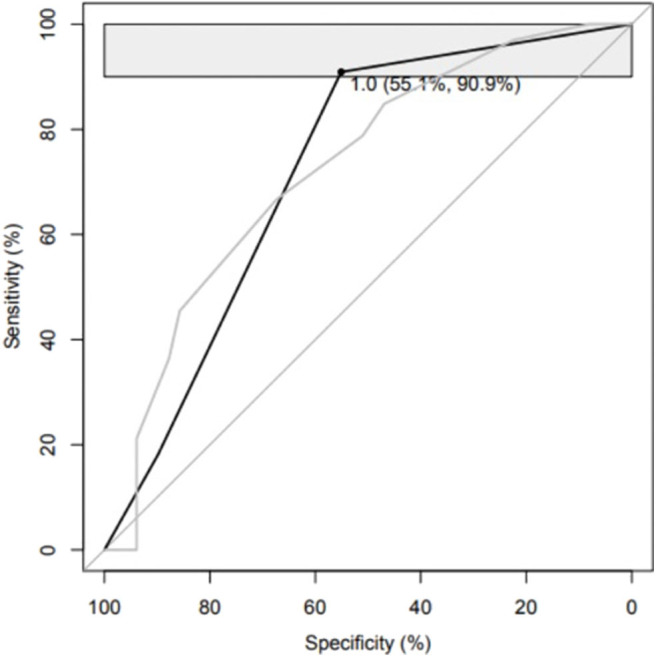
Blood biomarkers may enhance outcome prediction performance of head computed tomography scores in traumatic brain injury (TBI). To investigate whether admission levels of eight different protein biomarkers can improve the outcome prediction performance of the Helsinki computed tomography score (HCTS) without clinical covariates in TBI. Eighty-two patients with computed tomography positive TBIs were included in this study. Plasma levels of β-amyloid isoforms 1-40 (Aβ40) and 1-42 (Aβ42), glial fibrillary acidic protein, heart fatty acid-binding protein, interleukin 10 (IL-10), neurofilament light, S100 calcium-binding protein B, and total tau were measured within 24 h from admission. The patients were divided into favorable (Glasgow Outcome Scale-Extended 5-8, = 49) and unfavorable (Glasgow Outcome Scale-Extended 1-4, = 33) groups. The outcome was assessed 6-12 months after injury. An optimal predictive panel was investigated with the sensitivity set at 90-100%. The HCTS alone yielded a sensitivity of 97.0% (95% CI: 90.9-100) and specificity of 22.4% (95% CI: 10.2-32.7) and partial area under the curve of the receiver operating characteristic of 2.5% (95% CI: 1.1-4.7), in discriminating patients with favorable and unfavorable outcomes. The threshold to detect a patient with unfavorable outcome was an HCTS > 1. The three best individually performing biomarkers in outcome prediction were Aβ40, Aβ42, and neurofilament light. The optimal panel included IL-10, Aβ40, and the HCTS reaching a partial area under the curve of the receiver operating characteristic of 3.4% (95% CI: 1.7-6.2) with a sensitivity of 90.9% (95% CI: 81.8-100) and specificity of 59.2% (95% CI: 40.8-69.4). Admission plasma levels of IL-10 and Aβ40 significantly improve the prognostication ability of the HCTS after TBI.
血液生物标志物可能会提高创伤性脑损伤(TBI)中头部计算机断层扫描评分的预后预测性能。为了研究八种不同蛋白质生物标志物的入院水平是否能在不考虑临床协变量的情况下提高TBI中赫尔辛基计算机断层扫描评分(HCTS)的预后预测性能。本研究纳入了82例计算机断层扫描阳性的TBI患者。在入院后24小时内测量血浆中β-淀粉样蛋白亚型1-40(Aβ40)和1-42(Aβ42)、胶质纤维酸性蛋白、心脏脂肪酸结合蛋白、白细胞介素10(IL-10)、神经丝轻链、S100钙结合蛋白B和总tau的水平。患者被分为预后良好组(格拉斯哥预后量表扩展版5-8,n = 49)和预后不良组(格拉斯哥预后量表扩展版1-4,n = 33)。在受伤后6-12个月评估预后。研究了一个最佳预测指标组合,将敏感性设定为90%-100%。单独使用HCTS在区分预后良好和预后不良的患者时,敏感性为97.0%(95%CI:90.9-100),特异性为22.4%(95%CI:10.2-32.7),受试者操作特征曲线下的部分面积为2.5%(95%CI:1.1-4.7)。检测预后不良患者的阈值是HCTS>1。在预后预测中个体表现最佳的三种生物标志物是Aβ40、Aβ42和神经丝轻链。最佳指标组合包括IL-10、Aβ40和HCTS,受试者操作特征曲线下的部分面积为3.4%(95%CI:1.7-6.2),敏感性为90.9%(95%CI:81.8-100),特异性为59.2%(95%CI:40.8-69.4)。入院时血浆中IL-10和Aβ40水平显著提高了TBI后HCTS的预后预测能力。