Department of Pathology and Laboratory Medicine and UNC Blood Research Center, University of North Carolina, Chapel Hill (E.G.B., L.A.H., A.S.W.).
University of Utah Molecular Medicine Program, Salt Lake City, UT (F.D., A.M.B., M.T.R., R.A.C.).
Arterioscler Thromb Vasc Biol. 2021 Jan;41(1):401-414. doi: 10.1161/ATVBAHA.120.315338. Epub 2020 Nov 16.
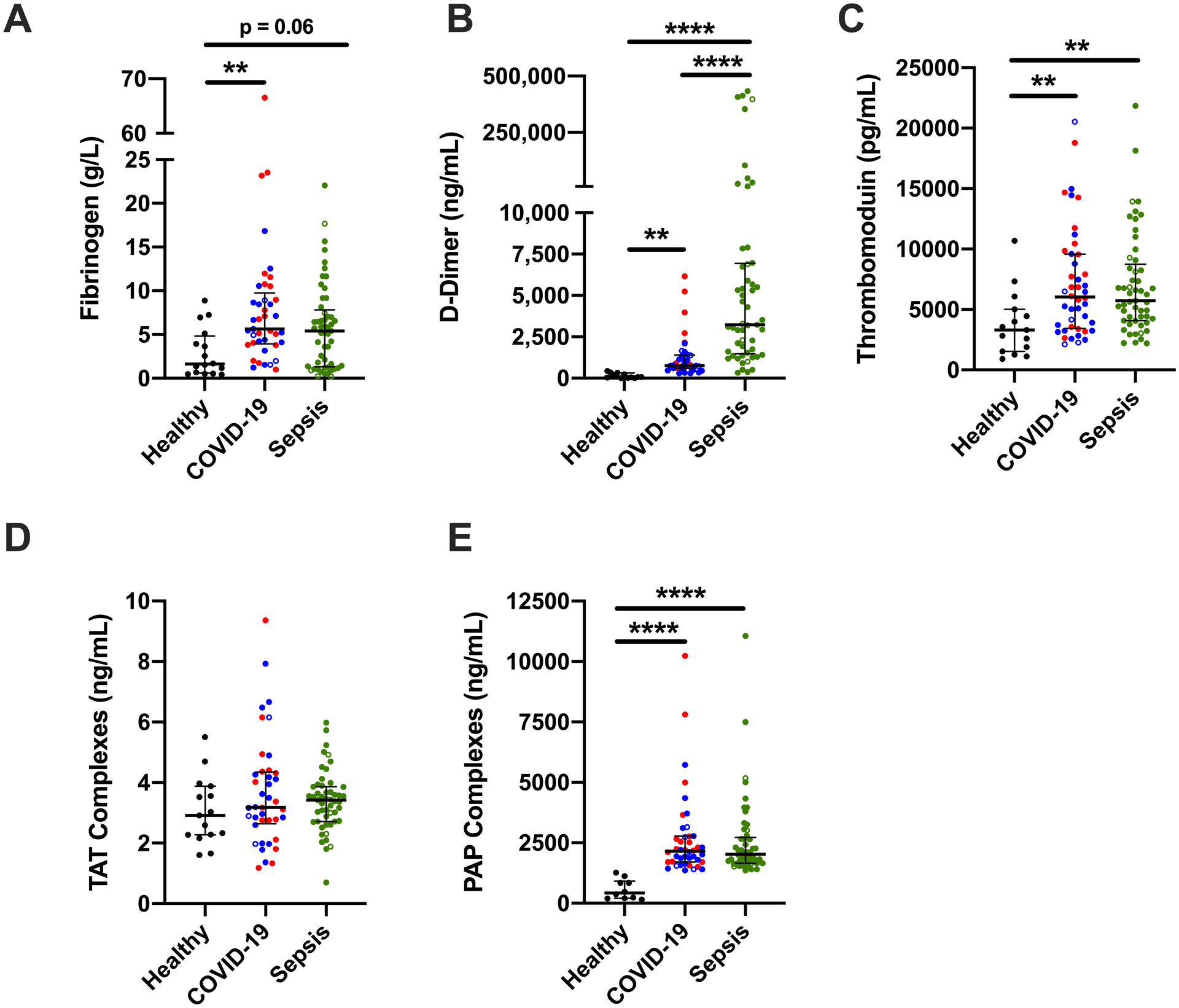
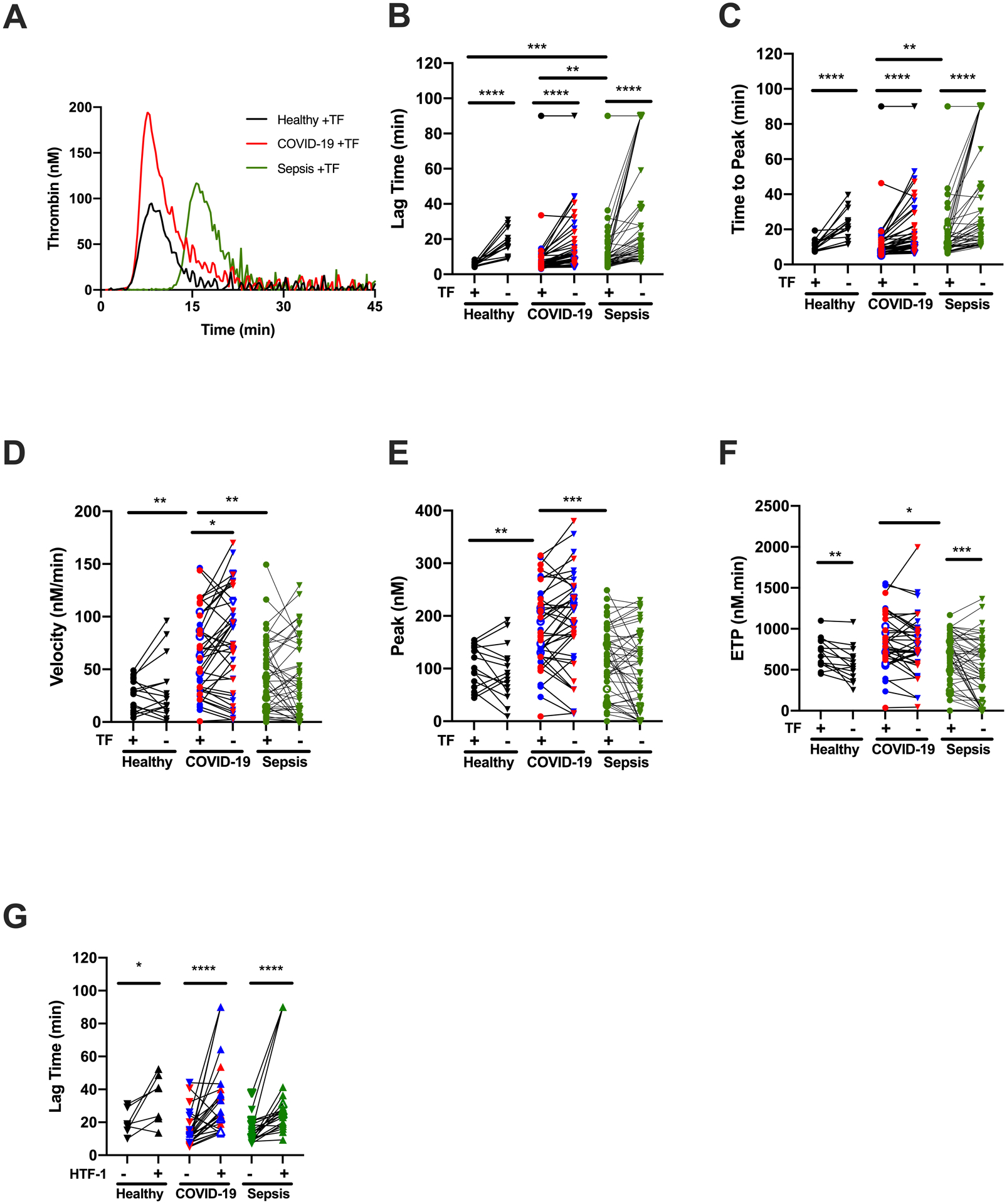
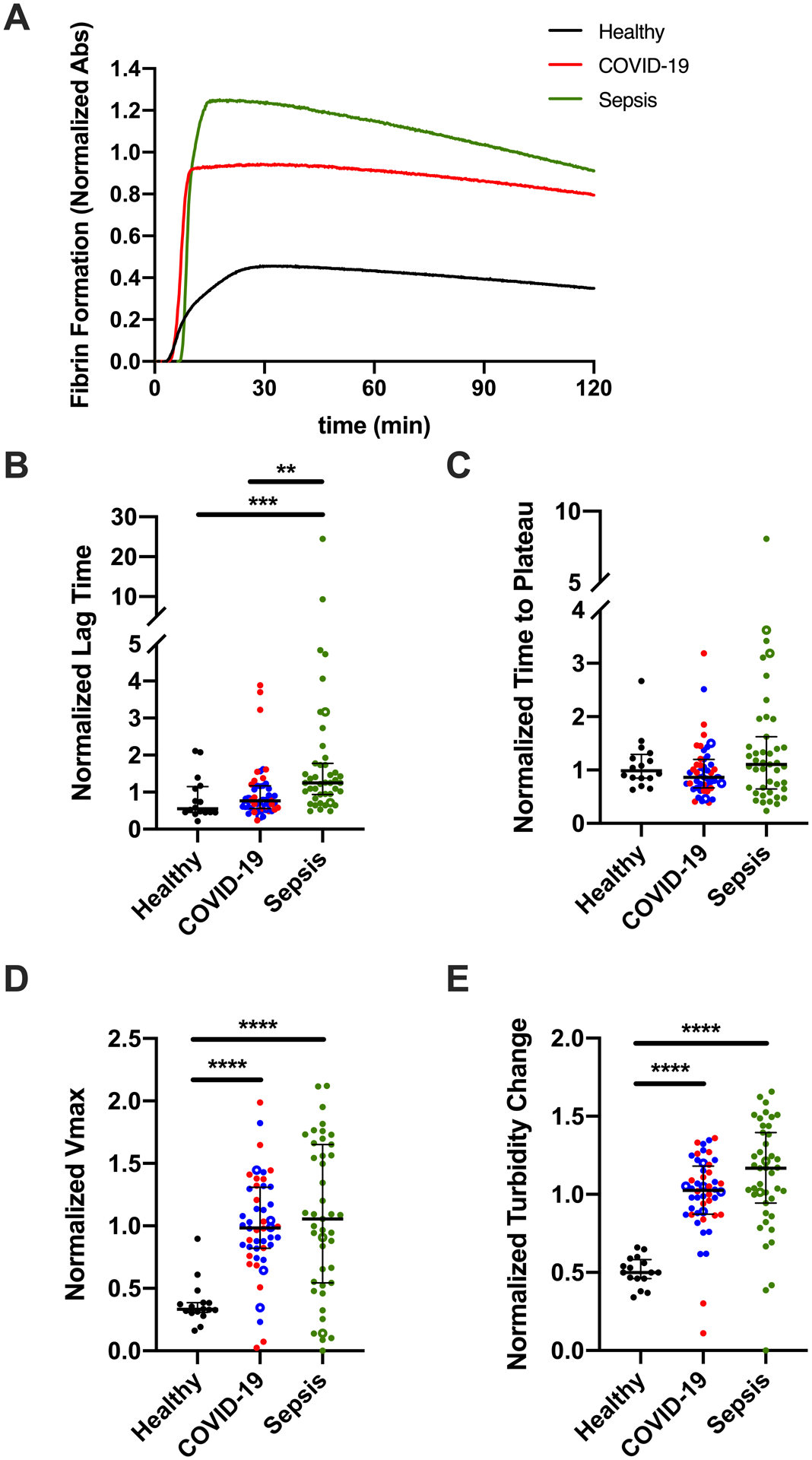
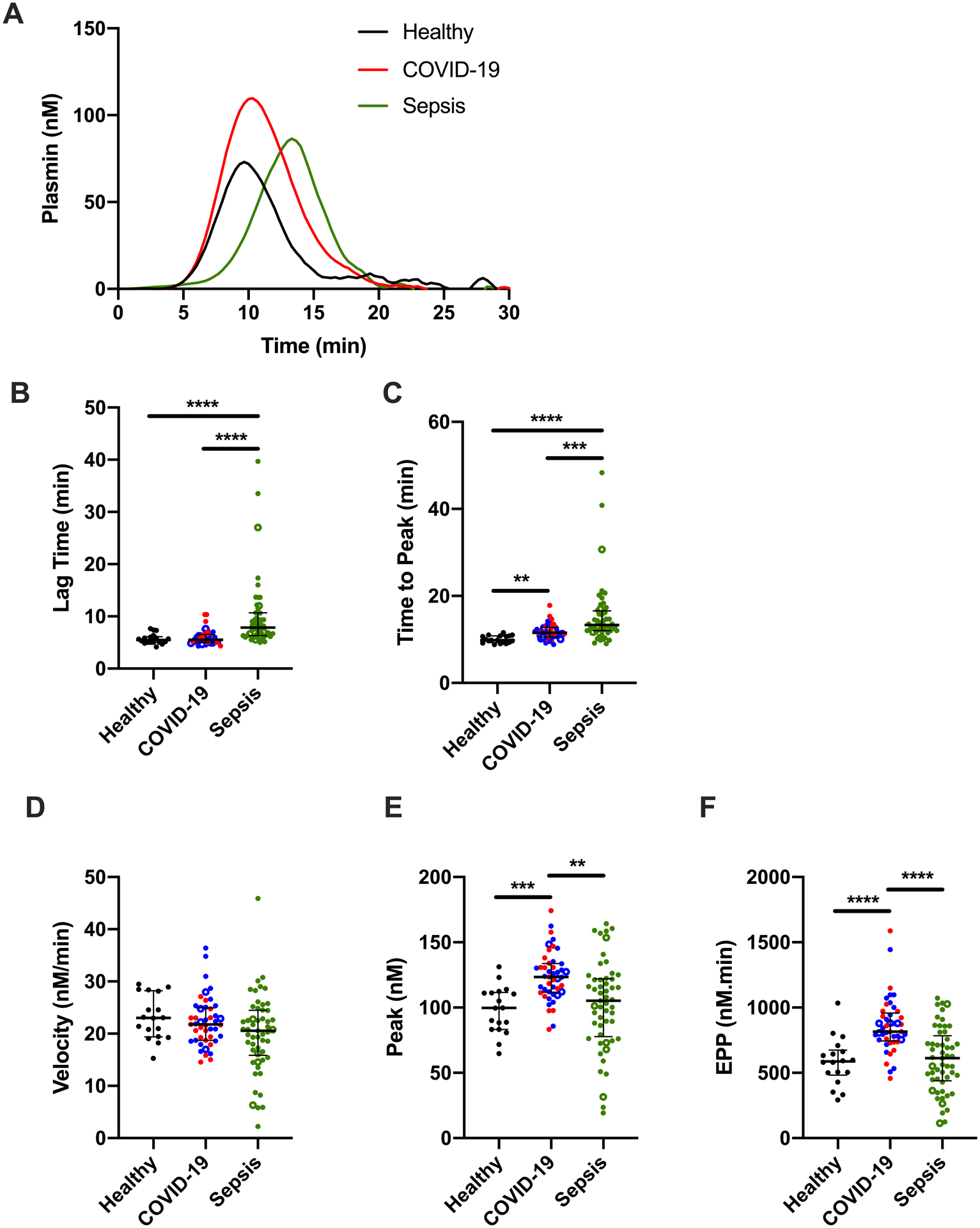
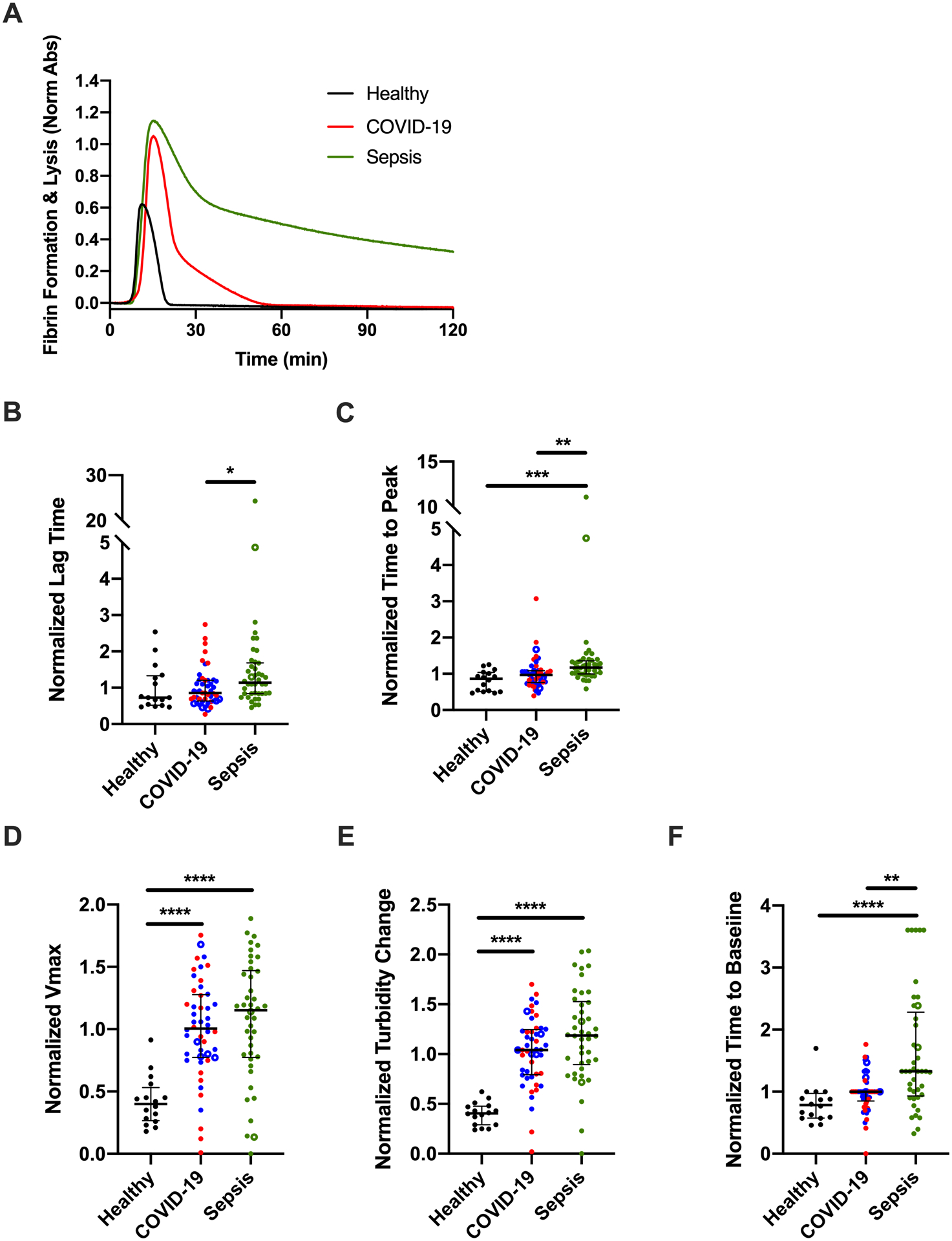
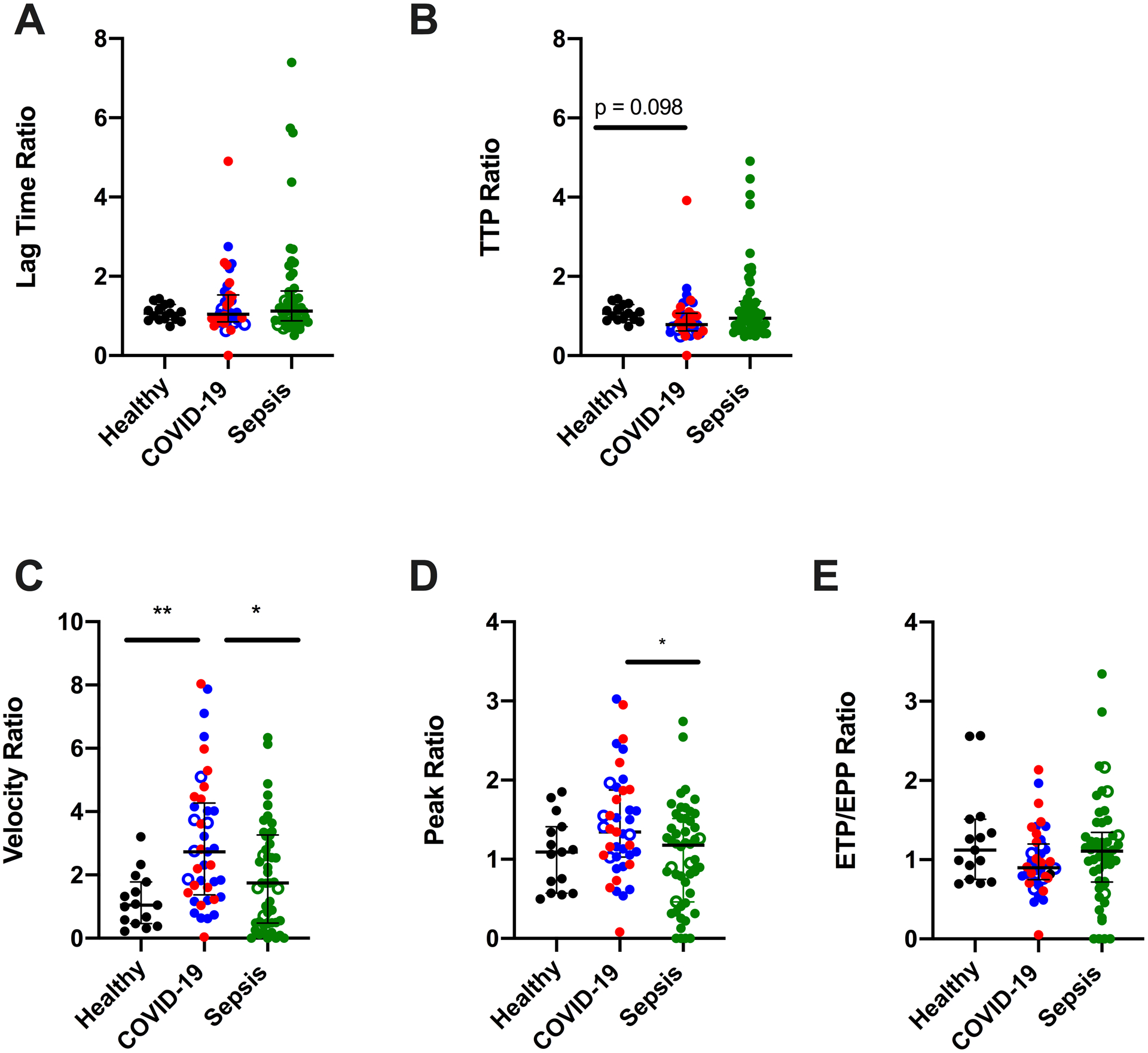
Coronavirus disease 2019 (COVID-19) is associated with derangement in biomarkers of coagulation and endothelial function and has been likened to the coagulopathy of sepsis. However, clinical laboratory metrics suggest key differences in these pathologies. We sought to determine whether plasma coagulation and fibrinolytic potential in patients with COVID-19 differ compared with healthy donors and critically ill patients with sepsis. Approach and Results: We performed comparative studies on plasmas from a single-center, cross-sectional observational study of 99 hospitalized patients (46 with COVID-19 and 53 with sepsis) and 18 healthy donors. We measured biomarkers of endogenous coagulation and fibrinolytic activity by immunoassays, thrombin, and plasmin generation potential by fluorescence and fibrin formation and lysis by turbidity. Compared with healthy donors, patients with COVID-19 or sepsis both had elevated fibrinogen, d-dimer, soluble TM (thrombomodulin), and plasmin-antiplasmin complexes. Patients with COVID-19 had increased thrombin generation potential despite prophylactic anticoagulation, whereas patients with sepsis did not. Plasma from patients with COVID-19 also had increased endogenous plasmin potential, whereas patients with sepsis showed delayed plasmin generation. The collective perturbations in plasma thrombin and plasmin generation permitted enhanced fibrin formation in both COVID-19 and sepsis. Unexpectedly, the lag times to thrombin, plasmin, and fibrin formation were prolonged with increased disease severity in COVID-19, suggesting a loss of coagulation-initiating mechanisms accompanies severe COVID-19.
Both COVID-19 and sepsis are associated with endogenous activation of coagulation and fibrinolysis, but these diseases differently impact plasma procoagulant and fibrinolytic potential. Dysregulation of procoagulant and fibrinolytic pathways may uniquely contribute to the pathophysiology of COVID-19 and sepsis.
新型冠状病毒病 2019(COVID-19)与凝血和血管内皮功能生物标志物的紊乱有关,其被比作脓毒症的凝血异常。然而,临床实验室指标表明这些病理存在关键差异。我们试图确定 COVID-19 患者的血浆凝血和纤维蛋白溶解潜能是否与健康供体和患有脓毒症的危重患者不同。
我们对来自单中心、横断性观察性研究的 99 名住院患者(46 名 COVID-19 患者和 53 名脓毒症患者)和 18 名健康供体的血浆进行了比较研究。我们通过免疫测定、荧光法测定凝血酶和纤溶酶生成潜能、浊度法测定纤维蛋白形成和溶解来测量内源性凝血和纤维蛋白溶解活性的生物标志物。与健康供体相比,COVID-19 或脓毒症患者的纤维蛋白原、D-二聚体、可溶性 TM(血栓调节蛋白)和纤溶酶-抗纤溶复合物均升高。尽管进行了预防性抗凝,但 COVID-19 患者的凝血酶生成潜能增加,而脓毒症患者则没有。COVID-19 患者的血浆还具有增加的内源性纤溶酶潜能,而脓毒症患者的纤溶酶生成延迟。在 COVID-19 和脓毒症中,血浆凝血酶和纤溶酶生成的集体扰动允许增强纤维蛋白形成。出乎意料的是,COVID-19 患者的凝血酶、纤溶酶和纤维蛋白形成的滞后时间随着疾病严重程度的增加而延长,这表明严重 COVID-19 伴随凝血起始机制的丧失。
COVID-19 和脓毒症均与内源性凝血和纤维蛋白溶解的激活有关,但这两种疾病对血浆促凝和纤维蛋白溶解潜能的影响不同。促凝和纤维蛋白溶解途径的失调可能是 COVID-19 和脓毒症病理生理学的独特贡献。