Global Clinical Development, Regeneron Pharmaceuticals Inc, Tarrytown, New York, USA.
Department of Rheumatology, Altoona Center for Research, Duncansville, Pennsylvania, USA.
Ann Rheum Dis. 2021 Apr;80(4):509-517. doi: 10.1136/annrheumdis-2020-217259. Epub 2020 Nov 16.
To study the efficacy and safety of fasinumab in moderate-to-severe, chronic low back pain (CLBP).
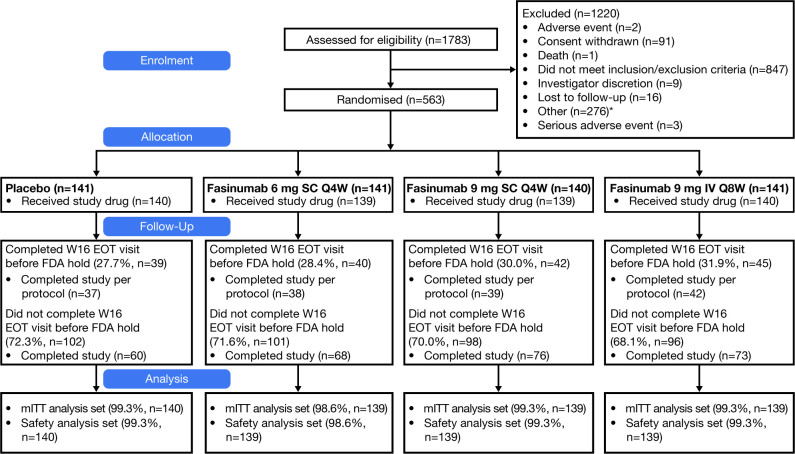
In this phase II/III, double-blind, placebo-controlled study, patients with CLBP aged ≥35 years with inadequate pain relief/intolerance to acetaminophen, non-steroidal anti-inflammatory drugs and opioids were randomised to fasinumab 6 or 9 mg subcutaneous every 4 weeks (Q4W), 9 mg intravenous every 8 weeks (Q8W) or placebo. Primary endpoint was change from baseline to week 16 in average daily low back pain intensity (LBPI) numeric rating score. Key secondary efficacy variables included Roland-Morris Disability Questionnaire (RMDQ) and Patient Global Assessment (PGA). The results are based on a modified intent-to-treat analysis of 563/800 planned patients when enrolment was stopped early given emerging signals of joint risk in other osteoarthritis (OA) studies at doses being tested here.
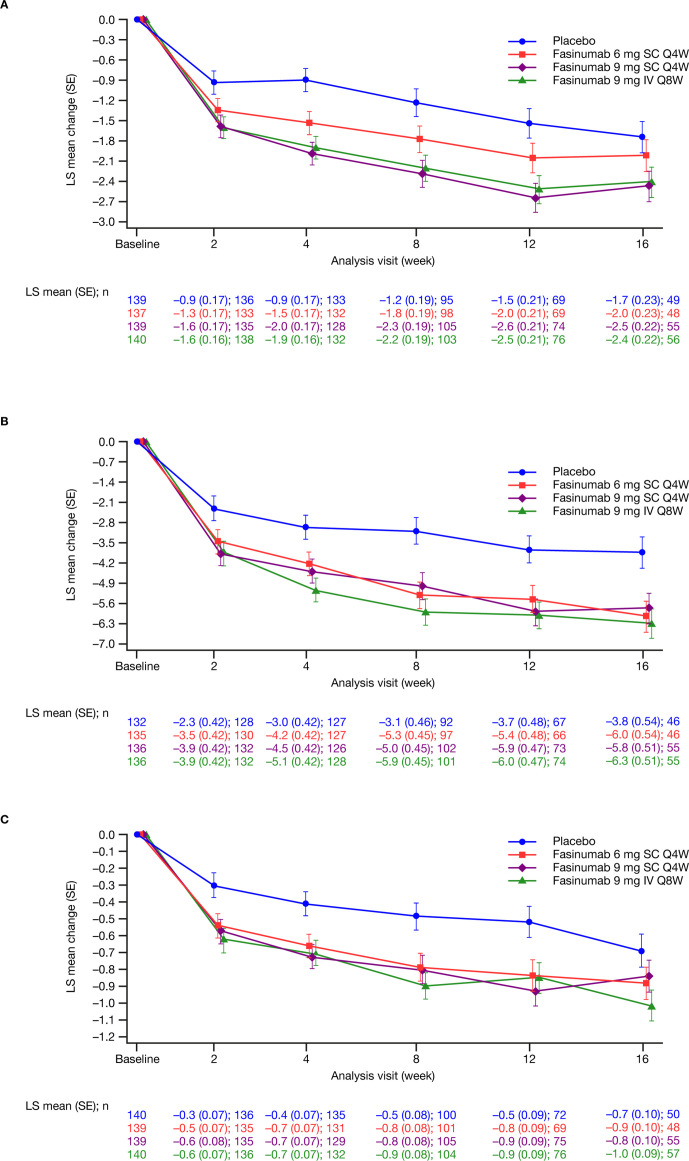
Significant placebo-adjusted LBPI reductions at week 16 were observed for fasinumab 9 mg Q4W and Q8W (least squares mean (standard error) -0.7 (0.3); both nominal p<0.05), but not 6 mg (-0.3 (0.3); p=0.39). RMDQ and PGA improvements to week 16 were greatest for fasinumab 9 mg intravenous. Numerically greater efficacy occurred in patients with, versus those without, peripheral OA (pOA) over 16 weeks. Treatment-emergent adverse events (AEs) occurred in 274/418 (65.6%) patients in the combined fasinumab groups and 94/140 (67.1%) placebo patients. Joint AEs, mostly rapid progressive OA type 1, were more frequent in the combined fasinumab groups (19 events in 16 patients (3.8%) vs 1 event in 1 patient (0.7%) for placebo); all except one occurred in pOA patients.
Fasinumab highest doses, but not lower dose, improved both CLBP pain and function. Most joint AEs occurred in pOA patients, consistent with earlier findings in symptomatic OA. Further study is needed of patients with CLBP with and without pOA to determine optimal benefit-risk.
研究 fasinumab 在中重度慢性下腰痛(CLBP)中的疗效和安全性。
这是一项 II/III 期、双盲、安慰剂对照研究,纳入年龄≥35 岁、对乙酰氨基酚、非甾体抗炎药和阿片类药物治疗反应不佳/不耐受的 CLBP 患者,随机接受 fasinumab 6 或 9mg 皮下注射,每 4 周 1 次(Q4W)、9mg 静脉注射,每 8 周 1 次(Q8W)或安慰剂治疗。主要终点为从基线到第 16 周时平均每日下腰痛强度(LBPI)数字评分的变化。关键次要疗效变量包括 Roland-Morris 残疾问卷(RMDQ)和患者整体评估(PGA)。这些结果基于对 800 名计划入组患者中的 563 名患者(当在剂量测试中发现其他骨关节炎 [OA] 研究中出现关节风险信号时,提前停止入组)进行的改良意向治疗分析。
在第 16 周时,fasinumab 9mg Q4W 和 Q8W 组与安慰剂组相比,LBPI 显著降低(最小二乘均数(标准误差)分别为-0.7(0.3)和-0.7(0.3);两者的 P 值均<0.05),而 6mg 组则无明显降低(-0.3(0.3);P=0.39)。在第 16 周时,fasinumab 9mg 静脉注射组的 RMDQ 和 PGA 改善程度最大。在 16 周内,外周性 OA(pOA)患者的疗效优于无 pOA 患者。在 fasinumab 联合治疗组和安慰剂组中,分别有 274/418(65.6%)和 94/140(67.1%)名患者发生治疗出现的不良事件(AEs)。联合 fasinumab 治疗组出现关节 AEs(主要为快速进展型 1 型 OA)的频率高于安慰剂组(16 名患者中有 19 例(3.8%),而安慰剂组中仅 1 名患者有 1 例(0.7%));除 1 例外,所有事件均发生在 pOA 患者中。
fasinumab 的高剂量(而非低剂量)可改善 CLBP 的疼痛和功能。大多数关节 AEs 发生在 pOA 患者中,与有症状性 OA 中的早期发现一致。需要进一步研究有和无 pOA 的 CLBP 患者,以确定最佳的获益-风险比。