Crohn-Colitis Centre, Bern, Switzerland.
Department of Gastroenterology, Clinic for Visceral Surgery and Medicine, Bern University Hospital, Bern, Switzerland.
United European Gastroenterol J. 2021 Apr;9(3):398-406. doi: 10.1177/2050640620965106. Epub 2021 Feb 26.
Vedolizumab (VDZ), a humanised monoclonal antibody against a4ß7-integrin, has shown efficacy in inflammatory bowel disease (IBD). It is of importance to assess the mid-to long-term efficacy of VDZ using real-life data.
Our study aimed to determine the efficacy of VDZ in patients with IBD with and without prior exposure to anti-tumour necrosis factor (TNF) treatments in a real-life setting. Furthermore, we investigated confounding factors influencing the remission to VDZ.
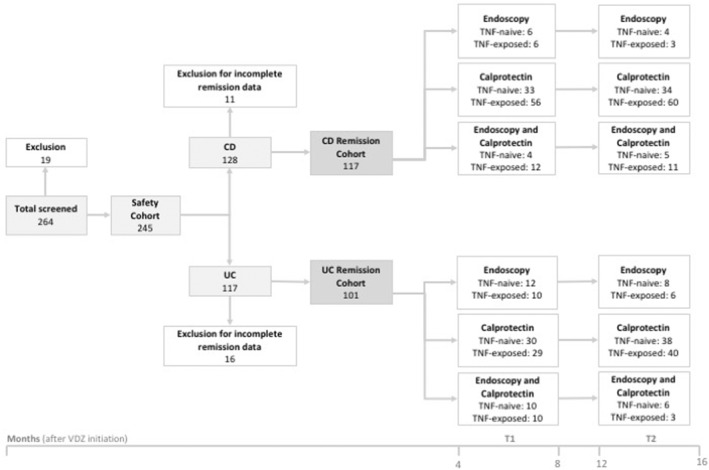
Patients participating in the Swiss IBD Cohort Study were included in this study. Remission was defined as calprotectin less than 200 mg/kg stool and/or mucosal healing determined by endoscopy. End points were determined between Months 4 and 8 (T1) and between Months 12 and 16 (T2) after VDZ induction.
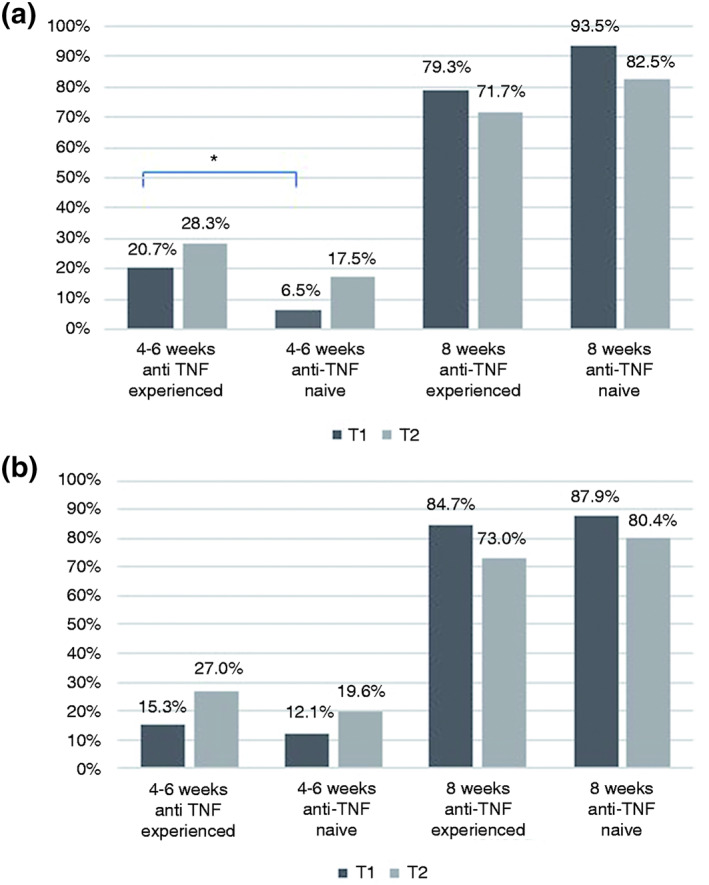
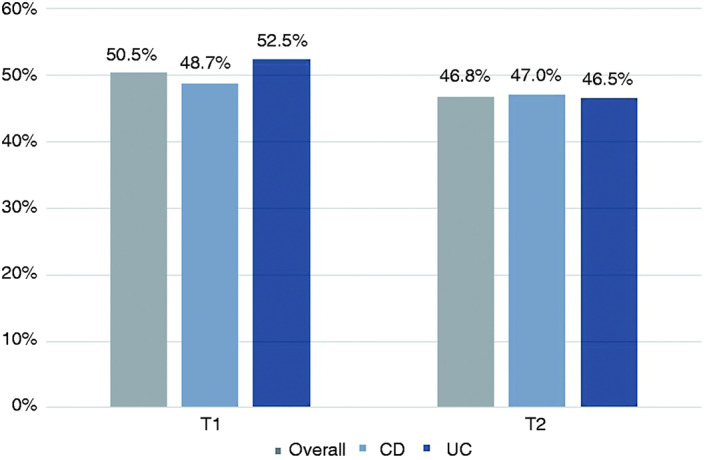
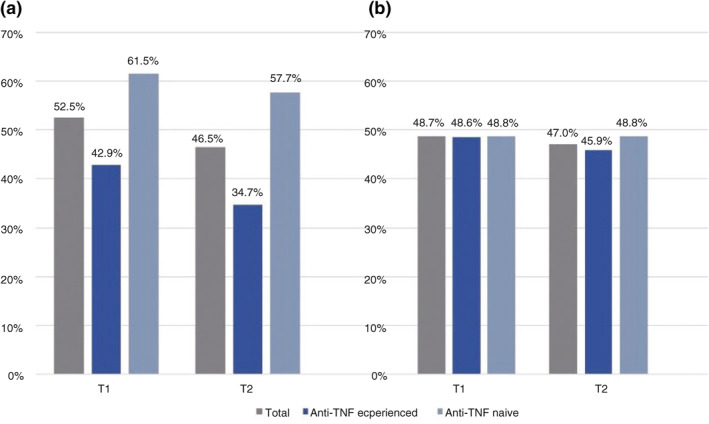
Remission was reported in 50.5% (110/218) of patients in T1 (48.7% Crohn's disease [CD] and 52.5% ulcerative colitis [UC]) and 46.8% (102/218) in T2 (47% CD and 46.5% UC). In UC patients, a significantly higher remission rate was achieved in T2 among anti-TNF-naive patients (57.7%) compared to anti-TNF-experienced patients (34.7%; p = 0.02; odds ratio = 0.39, 95% confidence interval: 0.17-0.87). In patients with CD, no difference could be seen in either evaluation interval. Multivariable analysis showed that disease duration significantly influenced remission rates among UC patients. A late response to VDZ therapy with an achievement of remission in T2 was seen in a fifth of all patients (CD: 21.7%, UC: 20.8%). VDZ treatment was stopped in a third of all patients (31.8%) due to nonresponse, adverse events or aggravation of extra-intestinal manifestations.
In a real-life national cohort setting, VDZ induced remission in more than half of IBD patients. Previous treatment with anti-TNF agents was associated with a significant lower efficacy of VDZ in UC but not in CD patients.
Vedolizumab(VDZ)是一种针对 a4ß7-整联蛋白的人源化单克隆抗体,已在炎症性肠病(IBD)中显示出疗效。使用真实数据评估 VDZ 的中至长期疗效非常重要。
本研究旨在确定 VDZ 在有和没有先前使用抗肿瘤坏死因子(TNF)治疗的 IBD 患者中的疗效,此外,我们还研究了影响 VDZ 缓解的混杂因素。
本研究纳入了参与瑞士 IBD 队列研究的患者。缓解定义为粪便钙卫蛋白<200mg/kg 和/或内镜下黏膜愈合。终点在 VDZ 诱导后 4 至 8 个月(T1)和 12 至 16 个月(T2)时确定。
T1 时,110/218 例(50.5%)患者报告缓解(48.7%克罗恩病[CD]和 52.5%溃疡性结肠炎[UC]),T2 时 102/218 例(46.8%)患者报告缓解(47%CD 和 46.5%UC)。在 UC 患者中,与抗 TNF 经验丰富的患者(34.7%)相比,抗 TNF 初治患者在 T2 时达到缓解的比例显著更高(57.7%;p=0.02;比值比=0.39,95%置信区间:0.17-0.87)。在 CD 患者中,两个评估间隔均未观察到差异。多变量分析显示,疾病持续时间显著影响 UC 患者的缓解率。所有患者中有五分之一(CD:21.7%,UC:20.8%)出现 VDZ 治疗的迟发反应,在 T2 时达到缓解。由于无反应、不良事件或肠外表现加重,所有患者中有三分之一(31.8%)停止了 VDZ 治疗。
在真实的全国队列环境中,VDZ 诱导了超过一半的 IBD 患者缓解。先前使用抗 TNF 药物与 UC 患者中 VDZ 疗效显著降低相关,但在 CD 患者中则无相关性。