Memorial Sloan Kettering Cancer Center, New York, New York.
Dana-Farber Cancer Institute, Boston, Massachusetts.
Clin Cancer Res. 2021 Feb 15;27(4):1019-1028. doi: 10.1158/1078-0432.CCR-20-3305. Epub 2020 Nov 17.
New therapies are needed to treat immune checkpoint inhibitor-resistant non-small cell lung cancer (NSCLC) and identify biomarkers to personalize treatment. Epigenetic therapies, including histone deacetylase inhibitors, may synergize with programmed cell death-1 (PD-1) blockade to overcome resistance. We report outcomes in patients with anti-programmed cell death ligand-1 [PD-(L)1]-resistant/refractory NSCLC treated with pembrolizumab plus entinostat in ENCORE 601.
The expansion cohort of ENCORE 601 included patients with NSCLC who previously experienced disease progression with immune checkpoint inhibitors. The primary endpoint for the phase II expansion cohort is overall response rate (ORR); safety, tolerability, and exploratory endpoints are described.
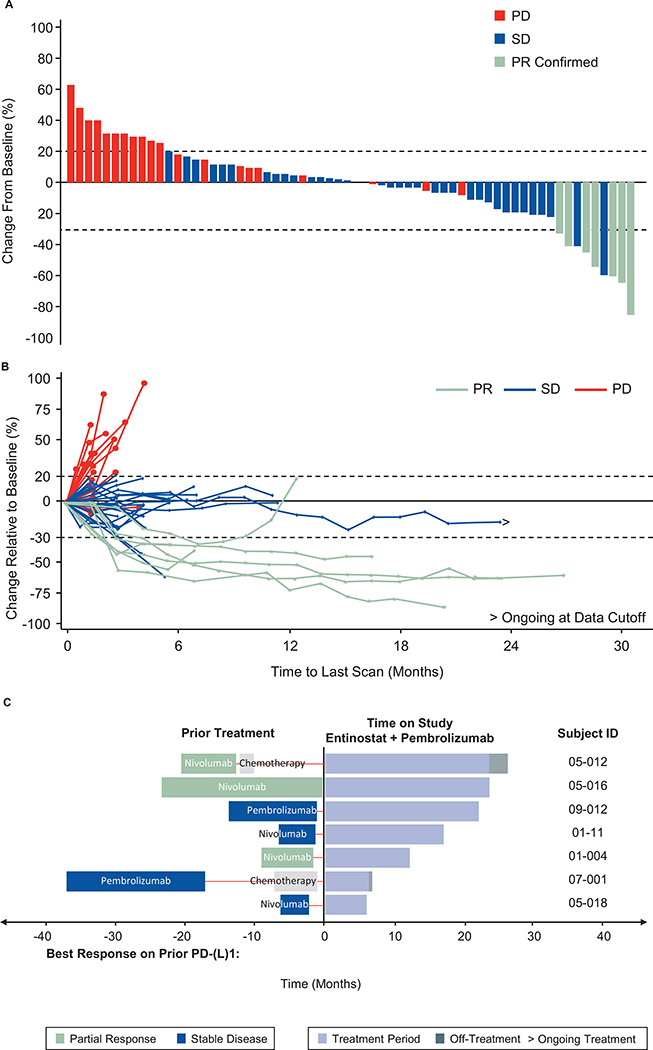
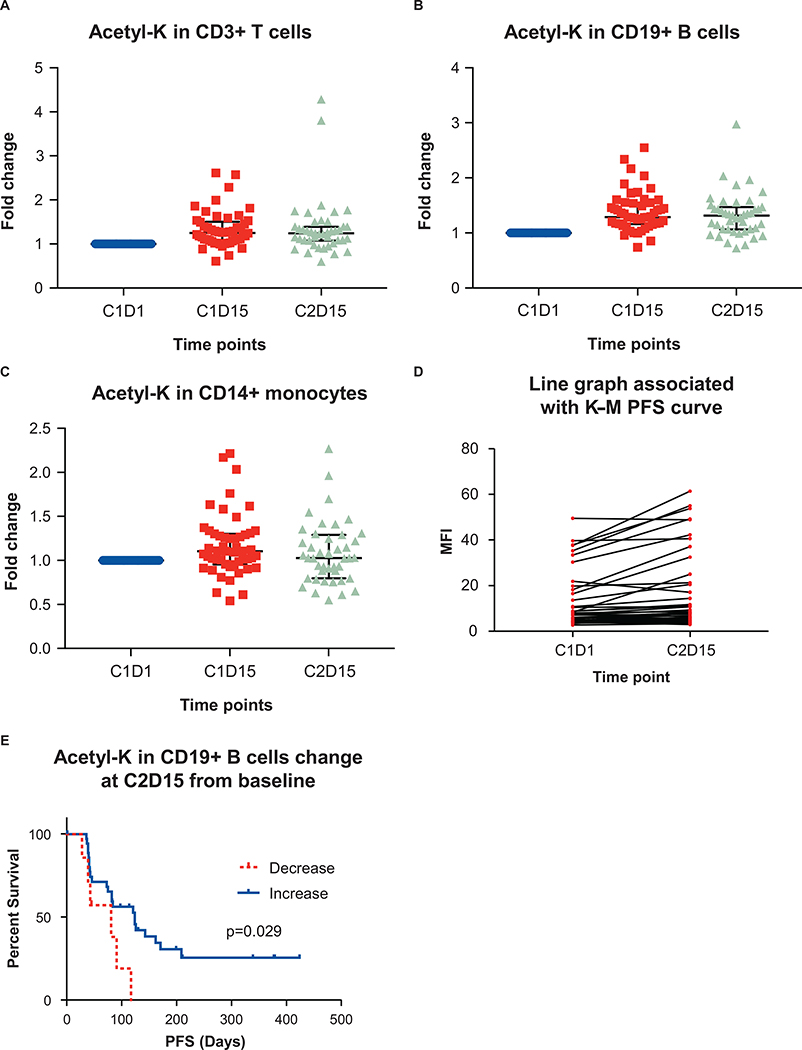
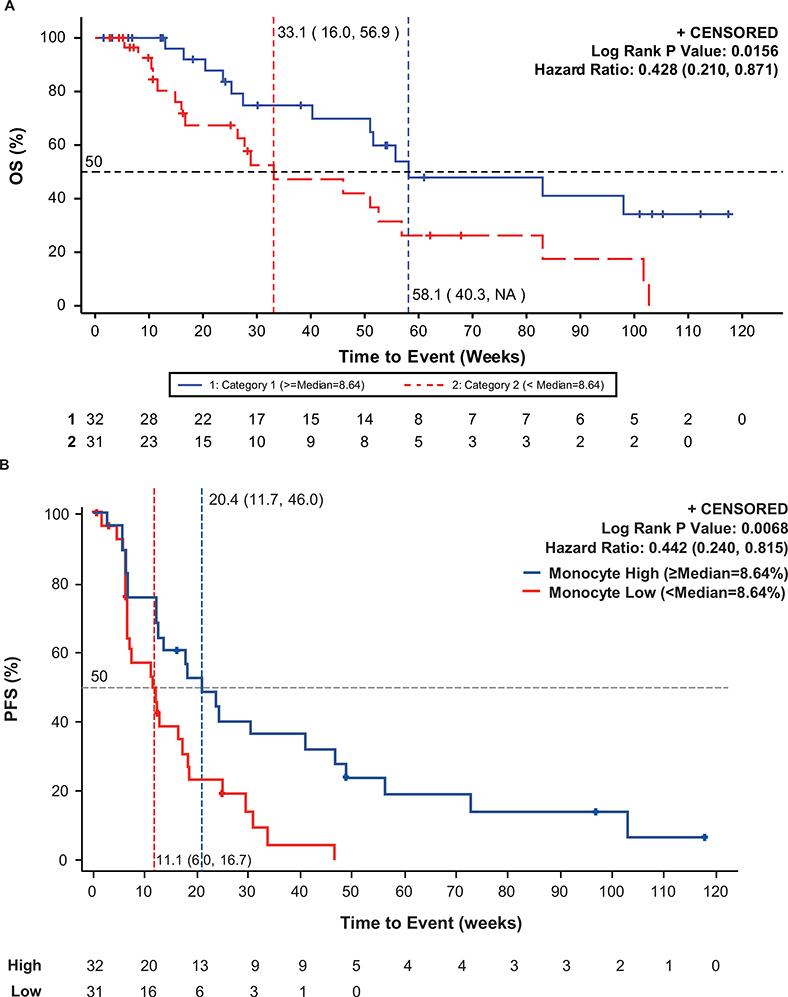
Of 76 treated patients, 71 were evaluable for efficacy. immune-regulated RECIST-assessed ORR was 9.2% [95% confidence interval (CI): 3.8-18.1], which did not meet the prespecified threshold for positivity. Median duration of response was 10.1 months (95% CI: 3.9-not estimable), progression-free survival (PFS) at 6 months was 22%, median PFS was 2.8 months (95% CI: 1.5-4.1), and median overall survival was 11.7 months (95% CI: 7.6-13.4). Benefit was enriched among patients with high levels of circulating classical monocytes at baseline. Baseline tumor PD-L1 expression and gene expression were not associated with benefit. Treatment-related grade ≥3 adverse events occurred in 41% of patients.
In anti-PD-(L)1-experienced patients with NSCLC, entinostat plus pembrolizumab did not achieve the primary response rate endpoint but provided a clinically meaningful benefit, with objective response in 9% of patients. No new toxicities, including immune-related adverse events, were seen for either drug. Future studies will continue to evaluate the association of monocyte levels and response.
需要新的疗法来治疗免疫检查点抑制剂耐药的非小细胞肺癌(NSCLC),并确定生物标志物来实现个体化治疗。表观遗传疗法,包括组蛋白去乙酰化酶抑制剂,可能与程序性细胞死亡-1(PD-1)阻断协同作用,以克服耐药性。我们报告了在接受派姆单抗联合恩替诺特治疗的抗程序性细胞死亡配体-1[PD-(L)1]耐药/难治性 NSCLC 患者中,ENCORE 601 中的患者的结果。
ENCORE 601 的扩展队列包括先前接受免疫检查点抑制剂治疗后疾病进展的 NSCLC 患者。该 II 期扩展队列的主要终点是总缓解率(ORR);描述了安全性、耐受性和探索性终点。
在 76 名接受治疗的患者中,71 名可评估疗效。免疫调节 RECIST 评估的 ORR 为 9.2%(95%CI:3.8-18.1),未达到阳性的预设阈值。中位缓解持续时间为 10.1 个月(95%CI:3.9-不可估计),6 个月时无进展生存期(PFS)为 22%,中位 PFS 为 2.8 个月(95%CI:1.5-4.1),中位总生存期为 11.7 个月(95%CI:7.6-13.4)。在基线时循环经典单核细胞水平较高的患者中,获益更为丰富。基线肿瘤 PD-L1 表达和基因表达与获益无关。41%的患者发生治疗相关的 3 级及以上不良事件。
在抗 PD-(L)1 经验的 NSCLC 患者中,恩替诺特联合派姆单抗未达到主要缓解率终点,但提供了有临床意义的获益,客观缓解率为 9%的患者。两种药物均未出现新的毒性反应,包括免疫相关不良事件。未来的研究将继续评估单核细胞水平与反应的相关性。