Chrysikos Serafeim, Gkiozos Ioannis, Dimakou Katerina, Zervas Eleftherios, Karampitsakos Theodoros, Anyfanti Maria, Tzouvelekis Argyrios, Samitas Konstantinos, Gaga Mina, Koulouris Nikolaos, Vasileiadis Ioannis, Syrigos Konstantinos
5 Respiratory Medicine Department, "Sotiria" Chest Diseases Hospital, Athens, Greece.
3 Internal Medicine Department, "Sotiria" Chest Diseases Hospital, Medical School, National and Kapodistrian University of Athens, Athens, Greece.
J Thorac Dis. 2020 Oct;12(10):5657-5666. doi: 10.21037/jtd-20-1735.
Accurate mediastinal staging in patients with non-small cell lung cancer (NSCLC) is crucial for the determination of optimal treatment management.
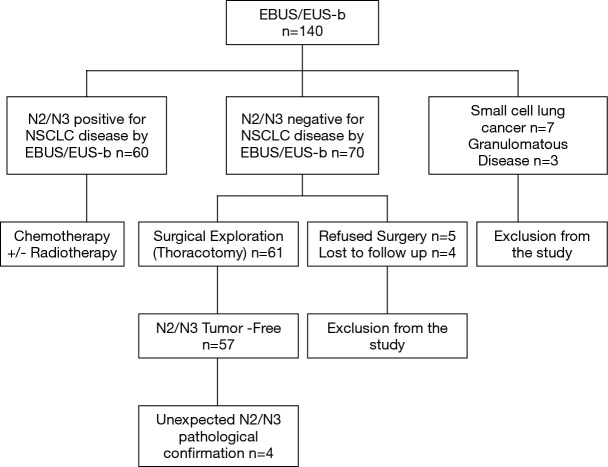
This was a real-life prospective study enrolling 140 patients between December 2016 and August 2018. We aimed to determine the clinical utility of EBUS/EUS-b in mediastinal staging of patients with NSCLC in comparison with integrated PET/CT. Furthermore, SUV cut-off value with the highest specificity/accuracy was evaluated. Subgroup analysis according to histological type was performed.
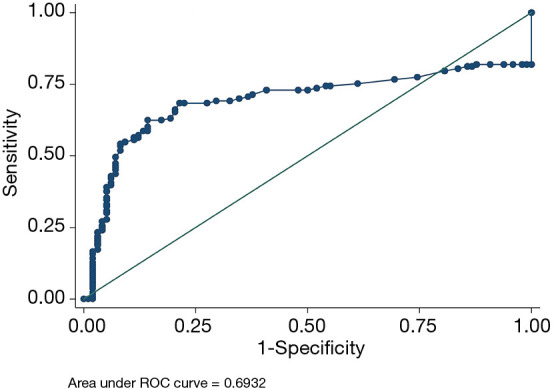
One hundred and thirty patients were eligible for analysis (mean age ± SD: 67.6±7.6, males 97). Three hundred different lymph node stations were sampled (272 through EBUS-TBNA and 28 through EUS-b FNA). Mean SUV of all malignant lymph nodes was 7.46 (SD =5.54). Sensitivity, specificity, PPV and NPV of EBUS/EUS-b for the identification of mediastinal malignant lymph nodes was 93.8%, 100%, 100%, and 93.4%, respectively. Accordingly, PET/CT yielded 92.2% sensitivity, 43.9% specificity, 64.8% PPV and 83.3% NPV. For adenocarcinoma (n=76) NPV were 86.2% with EBUS/EUS-b and 75% with PET/CT. NPV for squamous cell (n=46) was 100% with EBUS/EUS-b and 90.9% with PET/CT. EBUS/EUS-b staging yielded excellent agreement with final staging (97.5%, Tau 0.94, P<0.001). ROC curve analysis identified the value 4.95 as the optimal SUV cut-off value with the best specificity (87.4%) and accuracy (79%) (AUC 0.69; 95% CI: 0.73-0.84, P<0.001).
Thoracic endosonography is an excellent, minimally invasive tool yielding high sensitivity and diagnostic accuracy in mediastinal staging of patients with NSCLC. Implementation of both EBUS/EUS-b and PET/CT is necessary before any surgical intervention.
准确的非小细胞肺癌(NSCLC)患者纵隔分期对于确定最佳治疗方案至关重要。
这是一项在2016年12月至2018年8月期间纳入140例患者的真实前瞻性研究。我们旨在确定与PET/CT联合使用相比,EBUS/EUS-b在NSCLC患者纵隔分期中的临床应用价值。此外,还评估了具有最高特异性/准确性的SUV临界值。根据组织学类型进行亚组分析。
130例患者符合分析条件(平均年龄±标准差:67.6±7.6岁,男性97例)。共采集了300个不同的淋巴结站(272个通过EBUS-TBNA,28个通过EUS-b FNA)。所有恶性淋巴结的平均SUV为7.46(标准差=5.54)。EBUS/EUS-b识别纵隔恶性淋巴结的敏感性、特异性、阳性预测值和阴性预测值分别为93.8%、100%、100%和93.4%。相应地,PET/CT的敏感性为92.2%,特异性为43.9%,阳性预测值为64.8%,阴性预测值为83.3%。对于腺癌(n=76),EBUS/EUS-b的阴性预测值为86.2%,PET/CT为75%。鳞状细胞癌(n=46)的EBUS/EUS-b阴性预测值为100%,PET/CT为90.9%。EBUS/EUS-b分期与最终分期具有极好的一致性(97.5%,Tau 0.94,P<0.001)。ROC曲线分析确定4.95为最佳SUV临界值,具有最佳特异性(87.4%)和准确性(79%)(AUC 0.69;95%CI:0.73-0.84,P<0.001)。
胸部内镜超声是一种优秀的微创工具,在NSCLC患者纵隔分期中具有高敏感性和诊断准确性。在任何手术干预之前,同时实施EBUS/EUS-b和PET/CT是必要的。