Moon Youngkyu, Choi Si Young, Moon Mi Hyoung
Department of Thoracic & Cardiovascular Surgery, Eunpyeong St. Mary's Hospital, College of Medicine, The Catholic University of Korea, Seoul, Republic of Korea.
Department of Thoracic & Cardiovascular Surgery, Seoul St. Mary's Hospital, College of Medicine, The Catholic University of Korea, Seoul, Republic of Korea.
J Thorac Dis. 2020 Oct;12(10):5729-5738. doi: 10.21037/jtd-20-1840.
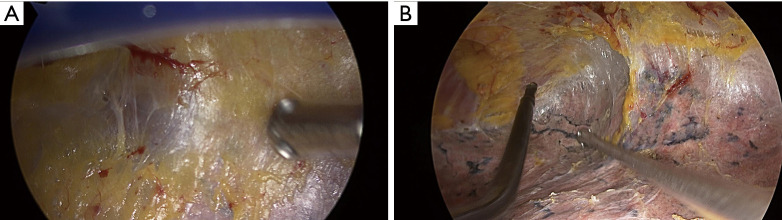
In cases of peripheral lung cancer with visceral pleural invasion and severe pleural adhesion, the question arises as to whether video-assisted thoracoscopic surgery (VATS) is a safe operation. The purpose of this study was to evaluate whether whole pleural adhesion is a risk factor for recurrence of cancer when performing VATS lobectomy for stage I non-small cell lung cancer (NSCLC) with visceral pleural invasion.
From 2010 to 2018, 123 consecutive patients who were diagnosed as stage I NSCLC with visceral pleural invasion and who underwent VATS lobectomy, were reviewed retrospectively. Those patients with partial pleural adhesion were excluded. The prognoses of the patients in the whole pleural adhesion group were compared with those of the non-adhesion group.
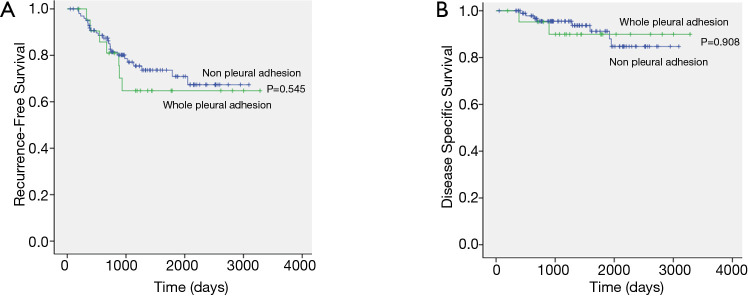
The clinicopathological characteristics were not found to differ between the two groups, with the exception of age. The mean age of the whole pleural adhesion group was found to be greater than that of the non-adhesion group (70.6 64.4, P=0.002). The 5-year recurrence-free survival rates for the whole pleural adhesion group and the non-adhesion group were 64.8% and 70.9% respectively, and they were not statistically different (P=0.545). In multivariate analysis, the extent of lymph node dissection (hazard ratio =13.854, P=0.023) was a significant risk factor for recurrence. Whole pleural adhesion was not a risk factor for recurrence.
Whole pleural adhesion was not a risk factor for recurrence after VATS lobectomy in stage I NSCLC with visceral pleural invasion. However, the extent of lymph node dissection was identified as an important prognostic factor.
对于伴有脏层胸膜侵犯和严重胸膜粘连的周围型肺癌患者,电视辅助胸腔镜手术(VATS)是否为安全的手术方式仍存在疑问。本研究旨在评估在对伴有脏层胸膜侵犯的I期非小细胞肺癌(NSCLC)行VATS肺叶切除术时,全胸膜粘连是否为癌症复发的危险因素。
回顾性分析2010年至2018年连续123例诊断为伴有脏层胸膜侵犯的I期NSCLC且接受VATS肺叶切除术的患者。排除部分胸膜粘连的患者。比较全胸膜粘连组与非粘连组患者的预后。
除年龄外,两组患者的临床病理特征未见差异。发现全胸膜粘连组的平均年龄大于非粘连组(70.6对64.4,P = 0.002)。全胸膜粘连组和非粘连组的5年无复发生存率分别为64.8%和70.9%,差异无统计学意义(P = 0.545)。多因素分析显示,淋巴结清扫范围(风险比=13.854,P = 0.023)是复发的重要危险因素。全胸膜粘连不是复发的危险因素。
对于伴有脏层胸膜侵犯的I期NSCLC患者,VATS肺叶切除术后全胸膜粘连不是复发的危险因素。然而,淋巴结清扫范围是一个重要的预后因素。