Interdisciplinary Consortium on Advanced Motion Performance, Division of Vascular Surgery and Endovascular Therapy, Michael E. DeBakey Department of Surgery, Baylor College of Medicine, Houston, Texas.
Keck School of Medicine, University of Southern California, Los Angeles.
JAMA Netw Open. 2020 Nov 2;3(11):e2020161. doi: 10.1001/jamanetworkopen.2020.20161.
Physical frailty is a key risk factor associated with higher rates of major adverse events (MAEs) after surgery. Assessing physical frailty is often challenging among patients with chronic limb-threatening ischemia (CLTI) who are often unable to perform gait-based assessments because of the presence of plantar wounds.
To test a frailty meter (FM) that does not rely on gait to determine the risk of occurrence of MAEs after revascularization for patients with CLTI.
DESIGN, SETTING, AND PARTICIPANTS: This cohort study included 184 consecutively recruited patients with CLTI at 2 tertiary care centers. After 32 individuals were excluded, 152 participants were included in the study. Data collection was conducted between May 2018 and June 2019.
Physical frailty measurement within 1 week before limb revascularization and incidence of MAEs for as long as 1 month after surgery.
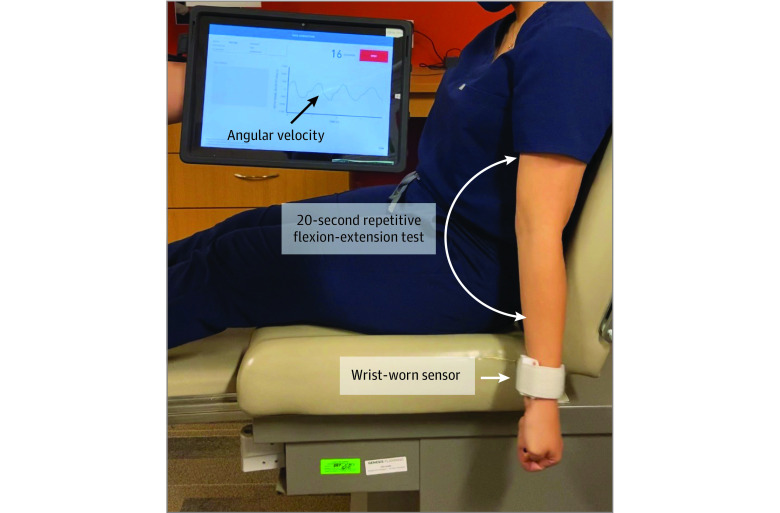
The FM works by quantifying weakness, slowness, rigidity, and exhaustion during a 20-second repetitive elbow flexion-extension exercise using a wrist-worn sensor. The FM generates a frailty index (FI) ranging from 0 to 1; higher values indicate progressively greater severity of physical frailty.
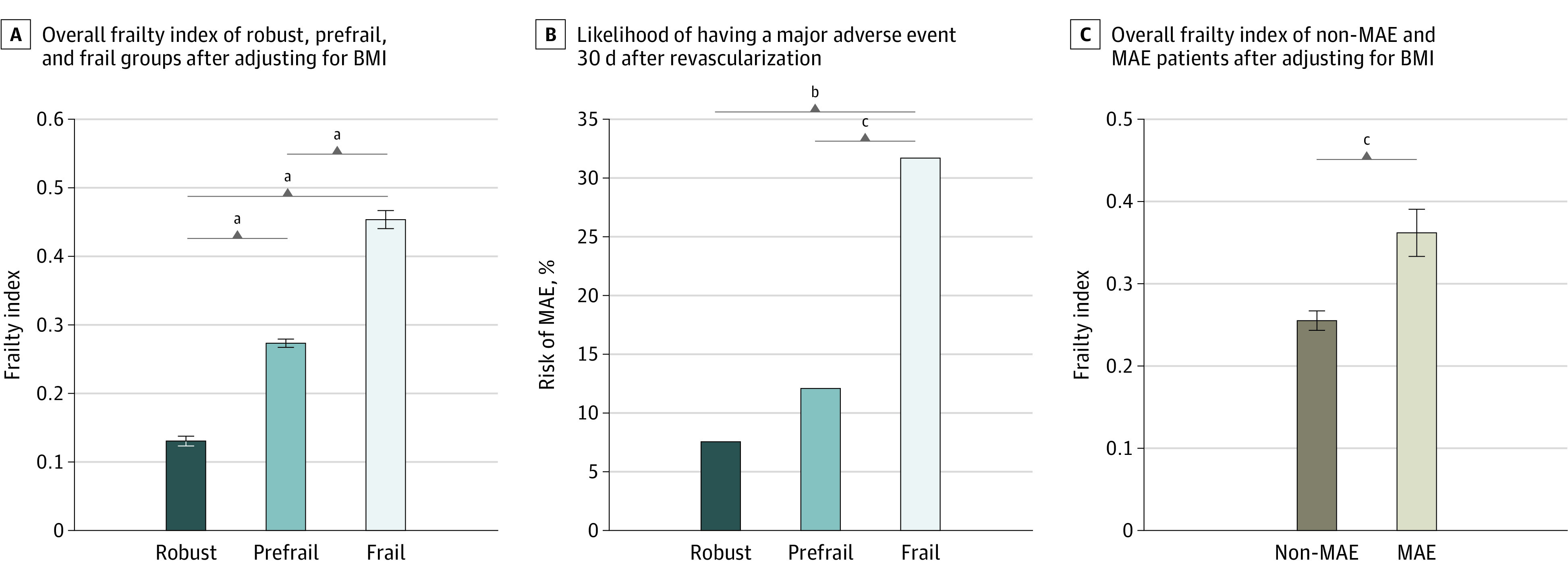
Of 152 eligible participants (mean [SD] age, 67.0 [11.8] years; 59 [38.8%] women), 119 (78.2%) were unable to perform the gait test, while all could perform the FM test. Overall, 53 (34.9%), 58 (38.1%), and 41 (27.0%) were classified as robust (FI <0.20), prefrail (FI ≥0.20 to <0.35), or frail (FI ≥0.35), respectively. Within 30 days after surgery, 24 (15.7%) developed MAEs, either major adverse cardiovascular events (MACE; 8 [5.2%]) or major adverse limb events (MALE; 16 [10.5%]). Baseline demographic characteristics were not significantly different between frailty groups. In contrast, the FI was approximately 30% higher in the group that developed MAEs (mean [SD] score, 0.36 [0.14]) than those who were MAE free (mean [SD] score, 0.26 [0.13]; P = .001), with observed MAE rates of 4 patients (7.5%), 7 patients (12.1%), and 13 patients (31.7%) in the robust, prefrail and frail groups, respectively (P = .004). The FI distinguished individuals who developed MACE and MALE from those who were MAE free (MACE: mean [SD] FI score, 0.38 [0.16]; P = .03; MALE: mean [SD] FI score, 0.35 [0.13]; P = .004) after adjusting by body mass index.
In this cohort study, measuring physical frailty using a wrist-worn sensor during a short upper extremity test was a practical method for stratifying the risk of MAEs following revascularization for CLTI when the administration of gait-based tests is often challenging.
身体虚弱是与手术后主要不良事件(MAE)发生率较高相关的关键风险因素。在患有慢性肢体威胁性缺血(CLTI)的患者中,评估身体虚弱通常具有挑战性,因为这些患者往往由于足底伤口的存在而无法进行基于步态的评估。
测试一种不需要依赖步态来确定 CLTI 患者血管重建后发生 MAE 风险的虚弱计(FM)。
设计、设置和参与者:这项队列研究纳入了 2 家三级护理中心的 184 名连续招募的 CLTI 患者。排除 32 人后,共有 152 名参与者纳入研究。数据收集于 2018 年 5 月至 2019 年 6 月进行。
肢体血运重建前 1 周内的身体虚弱测量和手术后 1 个月内 MAE 的发生率。
FM 通过使用手腕佩戴的传感器在 20 秒的重复肘部屈伸运动中量化虚弱、缓慢、僵硬和疲劳来工作。FM 生成一个虚弱指数(FI),范围从 0 到 1;更高的值表示身体虚弱的严重程度逐渐增加。
在 152 名符合条件的参与者中(平均[标准差]年龄,67.0[11.8]岁;59[38.8%]为女性),119 人(78.2%)无法进行步态测试,而所有人都可以进行 FM 测试。总体而言,分别有 53 人(34.9%)、58 人(38.1%)和 41 人(27.0%)被归类为强壮(FI<0.20)、衰弱前期(FI≥0.20 至<0.35)或衰弱(FI≥0.35)。术后 30 天内,24 人(15.7%)发生 MAE,要么是主要不良心血管事件(MACE;8[5.2%]),要么是主要不良肢体事件(MALE;16[10.5%])。基线人口统计学特征在脆弱组之间无显著差异。相比之下,发生 MAE 的组的 FI 约高出 30%(平均[标准差]评分,0.36[0.14]),而 MAE 阴性组的 FI 低约 30%(平均[标准差]评分,0.26[0.13];P=0.001),在强壮、衰弱前期和衰弱组中,发生 MAE 的发生率分别为 4 例(7.5%)、7 例(12.1%)和 13 例(31.7%)(P=0.004)。FI 区分了发生 MACE 和 MALE 的患者与 MAE 阴性的患者(MACE:平均[标准差]FI 评分,0.38[0.16];P=0.03;MALE:平均[标准差]FI 评分,0.35[0.13];P=0.004),在调整了体重指数后。
在这项队列研究中,使用手腕佩戴的传感器在短暂的上肢测试中测量身体虚弱是一种实用的方法,可以在进行基于步态的测试通常具有挑战性时,对 CLTI 血管重建后 MAE 的风险进行分层。