Grebmer Christian, Friedrich Lena, Semmler Verena, Kottmaier Marc, Bourier Felix, Brkic Amir, Blazek Patrick, Weigand Severin, Connor Matthew O', Deisenhofer Isabel, Hessling Gabriele, Kolb Christof, Lennerz Carsten
Deutsches Herzzentrum München, Klinik für Herz- uns Kreislauferkrankungen, Klinik an der Technischen Universität München, München, Germany; DZHK (German Centre for Cardiovascular Research), Partner Site Munich Heart Alliance, Munich, Germany.
Deutsches Herzzentrum München, Klinik für Herz- uns Kreislauferkrankungen, Klinik an der Technischen Universität München, München, Germany; DZHK (German Centre for Cardiovascular Research), Partner Site Munich Heart Alliance, Munich, Germany.
Indian Pacing Electrophysiol J. 2021 Jan-Feb;21(1):14-17. doi: 10.1016/j.ipej.2020.10.006. Epub 2020 Nov 17.
To evaluate whether left bundle branch block with residual conduction (rLBBB) is associated with worse outcomes after cardiac resynchronisation therapy (CRT).
All consecutive CRT implants at our institution between 2006 and 2013 were identified from our local device registry. Pre- and post-implant patient specific data were extracted from clinical records.
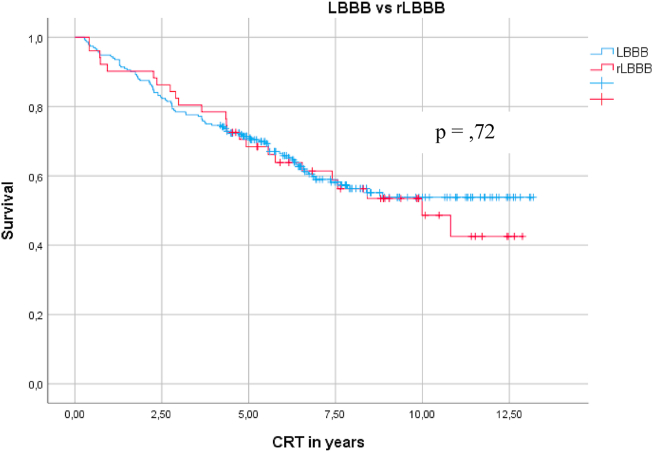
A total of 690 CRT implants were identified during the study period. Prior to CRT, 52.2% of patients had true left bundle branch block (LBBB), 19.1% a pacing-induced LBBB (pLBBB), 11.2% a rLBBB, 0.8% a right bundle branch block (RBBB), and 16.5% had a nonspecific intraventricular conduction delay (IVCD) electrocardiogram pattern. Mean age at implant was 67.5 years (standard deviation [SD] = 10.6), mean left ventricular ejection fraction (LV EF) was 25.7% (SD = 7.9%), and mean QRS duration was 158.4 ms (SD = 32 ms). After CRT, QRS duration was significantly reduced in the LBBB (p < 0.001), pLBBB (p < 0.001), rLBBB (p < 0.001), RBBB (p = 0.04), and IVCD groups (p = 0.03). LV EF significantly improved in the LBBB (p < 0.001), rLBBB (p = 0.002), and pLBBB (p < 0.001) groups, but the RBBB and IVCD groups showed no improvement. There was no significant difference in mortality between the LBBB and rLBBB groups. LV EF post-CRT, chronic kidney disease, hyperkalaemia, hypernatremia, and age at implant were significant predictors of mortality.
CRT in patients with rLBBB results in improved LV EF and similar mortality rates to CRT patients with complete LBBB. Predictors of mortality post-CRT include post-CRT LV EF, presence of CKD, hyperkalaemia, hypernatremia, and older age at implant.
评估伴有残余传导的左束支传导阻滞(rLBBB)是否与心脏再同步治疗(CRT)后更差的预后相关。
从我们当地的设备登记处识别出2006年至2013年间在我们机构进行的所有连续CRT植入病例。从临床记录中提取植入前后的患者特定数据。
在研究期间共识别出690例CRT植入病例。在CRT之前,52.2%的患者有真正的左束支传导阻滞(LBBB),19.1%为起搏诱导的LBBB(pLBBB),11.2%为rLBBB,0.8%为右束支传导阻滞(RBBB),16.5%的患者有非特异性室内传导延迟(IVCD)心电图模式。植入时的平均年龄为67.5岁(标准差[SD]=10.6),平均左心室射血分数(LV EF)为25.7%(SD=7.9%),平均QRS时限为158.4毫秒(SD=32毫秒)。CRT后,LBBB组(p<0.001)、pLBBB组(p<0.001)、rLBBB组(p<0.001)、RBBB组(p=0.04)和IVCD组(p=0.03)的QRS时限均显著缩短。LBBB组(p<0.001)、rLBBB组(p=0.002)和pLBBB组(p<0.001)的LV EF显著改善,但RBBB组和IVCD组无改善。LBBB组和rLBBB组之间的死亡率无显著差异。CRT后的LV EF、慢性肾脏病、高钾血症、高钠血症和植入时的年龄是死亡率的显著预测因素。
rLBBB患者的CRT可使LV EF改善,死亡率与完全性LBBB的CRT患者相似。CRT后死亡率的预测因素包括CRT后的LV EF、CKD的存在、高钾血症、高钠血症和植入时年龄较大。