Department of Oncology, Shandong First Medical University and Shandong Academy of Medical Sciences, Jinan, China.
Department of Radiation Oncology, Shandong Cancer Hospital and Institute, Shandong First Medical University and Shandong Academy of Medical Sciences, Jinan, China.
Front Immunol. 2020 Oct 30;11:580335. doi: 10.3389/fimmu.2020.580335. eCollection 2020.
The programmed cell death ligand 1 (PD-L1) plays a key role in glioma development. However, due to the specificity of glioma's anatomical position, the role of its expression as a tumor biomarker is limited. It has been proven that the levels of soluble programmed death-ligand 1 (sPD-L1) are associated with prognosis in many malignancies including glioma. However, the expression of sPD-L1 in glioma patients receiving radiotherapy (RT) remains unclear. The purpose of this study was to evaluate the concentration of sPD-L1 in the plasma of glioma patients before and after RT and to explore its relationship with clinical outcomes.
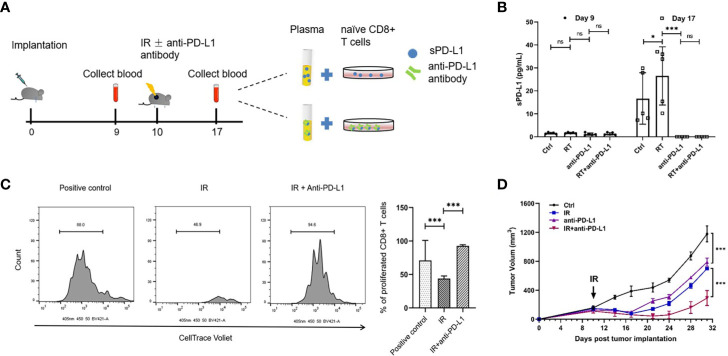
Between October 2017 and September 2018, glioma patients treated with RT (30 ± 10 Gy, 2 Gy/f) were enrolled, and blood samples were collected before and after RT. We quantified the sPD-L1 levels by enzyme-linked immunosorbent assay (ELISA). The isocitrate dehydrogenase-1 (IDH-1) mutational status and Ki-67 expression of tumors were evaluated by immunohistochemistry. Glioma murine model were used to address whether circulating sPD-L1 molecules are directly targeted by an anti-PD-L1 antibody. The associations between sPD-L1 and clinical features were assessed with Pearson's or Spearman's correlation analysis. The progression-free survival (PFS) and overall survival (OS) were determined by the Kaplan-Meier method.
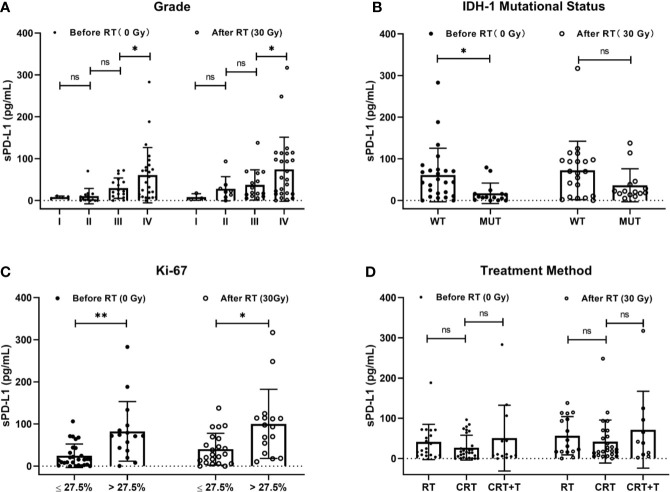
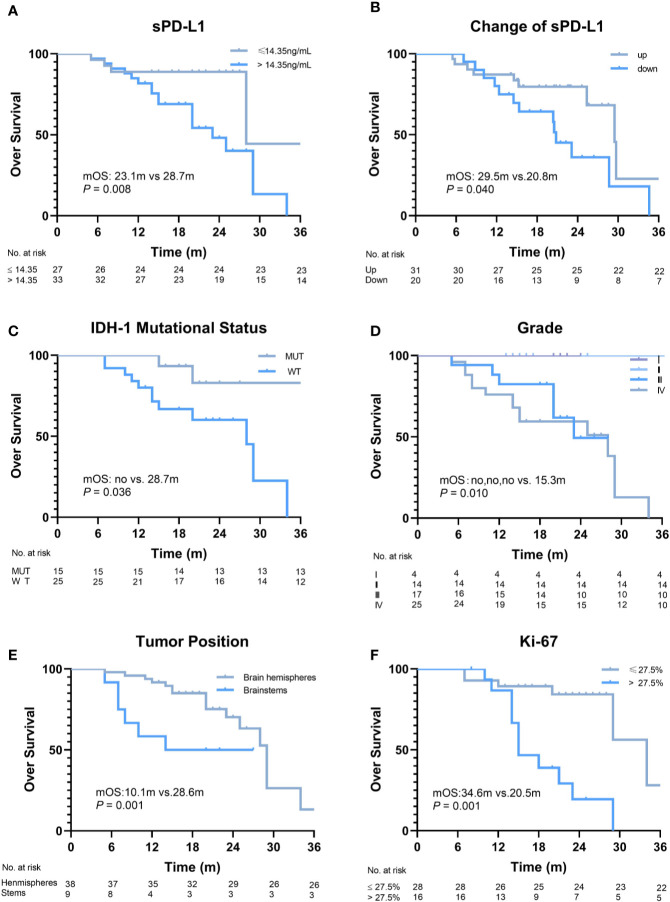
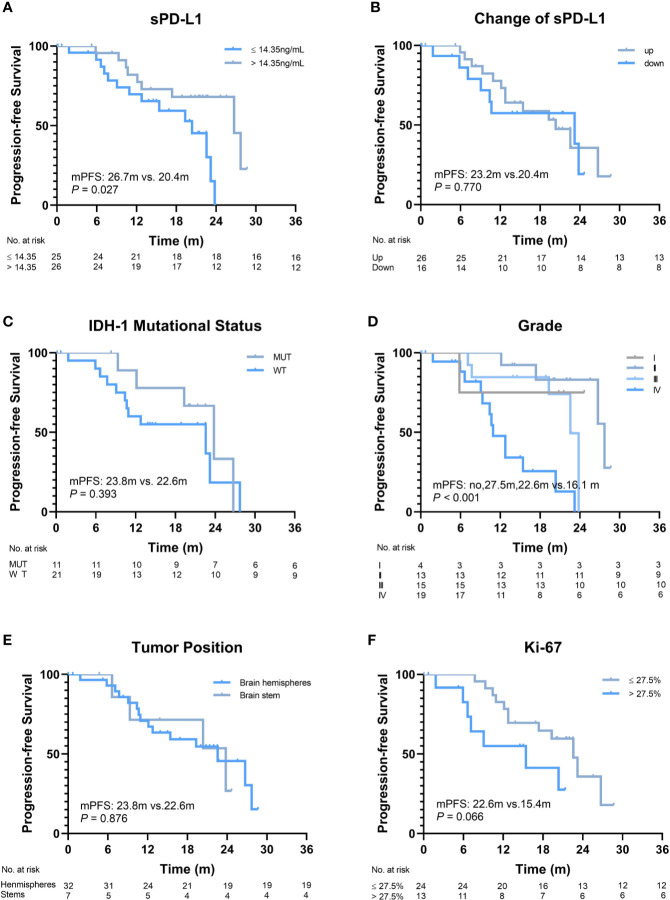
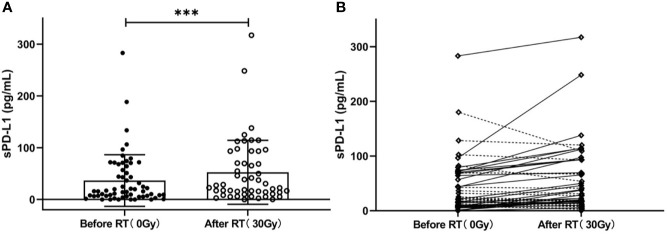
Sixty glioma patients were included, with a median age of 52 years. The proportions of grade I, II, III, and IV gliomas were 6.7%, 23.3%, 28.4%, and 41.6%, respectively. The baseline sPD-L1 levels were significantly associated with tumor grade, IDH-1 mutation status and Ki-67 expression. Using 14.35 pg/ml as the cutoff, significantly worse PFS and OS were both observed in patients with higher baseline levels of sPD-L1 ( = 0.027 and 0.008, respectively). RT significantly increased the mean level of sPD-L1 ( < 0.001). Further analysis showed that the level of sPD-L1 in IDH-1 mutation patients was higher than that in wild-type patients. Furthermore, an analysis of glioma murine model indicated that anti-PD-L1 antibody combine with RT can be a potentially powerful cancer therapy.
This study reported that sPD-L1 might be a potential biomarker to predict the outcome in glioma patients receiving RT. The elevated level of sPD-L1 after RT suggested that the strategy of a combination of immune checkpoint inhibitors and RT might be promising for glioma patients, especially for those with IDH-1 mutations.
程序性细胞死亡配体 1(PD-L1)在神经胶质瘤的发展中起着关键作用。然而,由于神经胶质瘤的解剖位置的特殊性,其表达作为肿瘤标志物的作用是有限的。已经证明,可溶性程序性死亡配体 1(sPD-L1)的水平与许多恶性肿瘤包括神经胶质瘤的预后相关。然而,接受放疗(RT)的神经胶质瘤患者的 sPD-L1 表达尚不清楚。本研究旨在评估神经胶质瘤患者在 RT 前后血浆中 sPD-L1 的浓度,并探讨其与临床结局的关系。
2017 年 10 月至 2018 年 9 月,纳入接受 RT(30±10Gy,2Gy/f)治疗的神经胶质瘤患者,并在 RT 前后采集血样。我们通过酶联免疫吸附试验(ELISA)定量 sPD-L1 水平。通过免疫组织化学评估肿瘤的异柠檬酸脱氢酶-1(IDH-1)突变状态和 Ki-67 表达。使用神经胶质瘤小鼠模型来解决循环 sPD-L1 分子是否直接被抗 PD-L1 抗体靶向。使用 Pearson 或 Spearman 相关分析评估 sPD-L1 与临床特征的相关性。使用 Kaplan-Meier 法确定无进展生存期(PFS)和总生存期(OS)。
纳入 60 例神经胶质瘤患者,中位年龄为 52 岁。I、II、III 和 IV 级神经胶质瘤的比例分别为 6.7%、23.3%、28.4%和 41.6%。基线 sPD-L1 水平与肿瘤分级、IDH-1 突变状态和 Ki-67 表达显著相关。以 14.35pg/ml 为截点,基线 sPD-L1 水平较高的患者 PFS 和 OS 均显著较差(=0.027 和 0.008,分别)。RT 显著增加了 sPD-L1 的平均水平(<0.001)。进一步分析表明,IDH-1 突变患者的 sPD-L1 水平高于野生型患者。此外,对神经胶质瘤小鼠模型的分析表明,抗 PD-L1 抗体联合 RT 可能是一种潜在有效的癌症治疗方法。
本研究报道 sPD-L1 可能是预测接受 RT 的神经胶质瘤患者预后的潜在生物标志物。RT 后 sPD-L1 水平升高提示免疫检查点抑制剂联合 RT 的策略可能对神经胶质瘤患者,特别是 IDH-1 突变患者有希望。