Weycker Derek, Moynahan Aaron, Silvia Amanda, Sato Reiko
Policy Analysis Inc. (PAI), 822 Boylston Street, Suite 206, Chestnut Hill, MA, 02467, USA.
Pfizer Inc., Collegeville, PA, USA.
Pharmacoecon Open. 2021 Jun;5(2):275-284. doi: 10.1007/s41669-020-00240-9. Epub 2020 Nov 23.
While much is known about the cost of community-acquired pneumonia (CAP) during the acute phase of illness, little is known about the potential attributable cost of CAP thereafter.
The aim of this study was to assess long-term attributable costs associated with CAP among adults in US clinical practice.
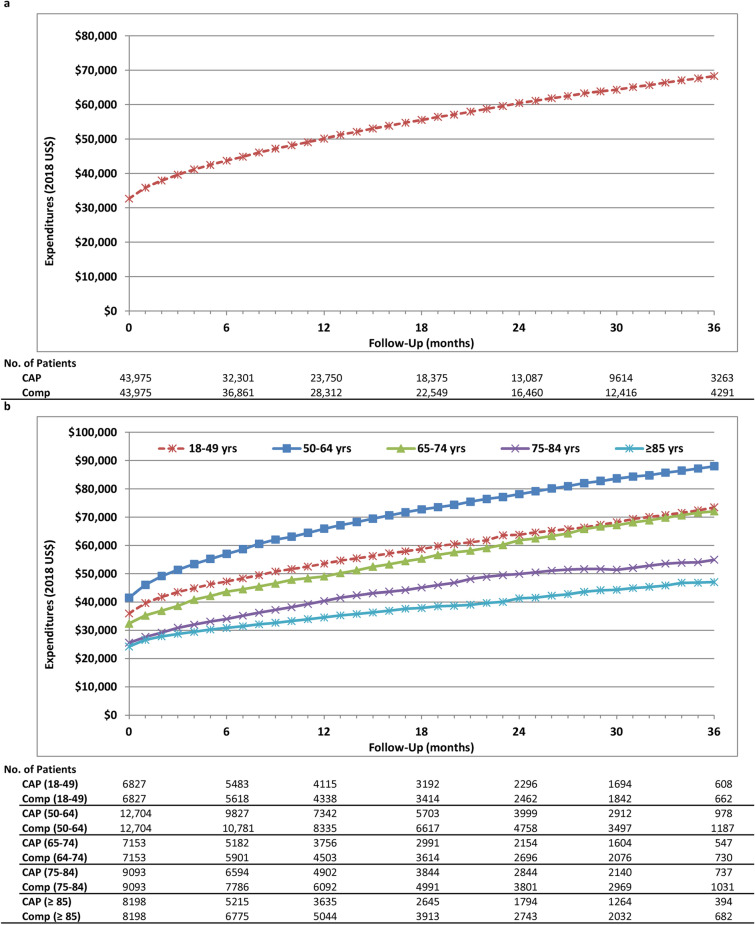
A retrospective matched cohort design and data from a US private healthcare claims repository were employed. In each month during the study period (2011-2016), adults who were hospitalized for CAP in that month ('CAP patients') were matched (1:1, without replacement) on demographic, clinical, and healthcare profiles to adults who did not develop CAP in that month ('comparison patients'). All-cause healthcare expenditures were tallied for the qualifying CAP hospitalization and during the 30-day period post-discharge (collectively, 'acute phase'), as well as from the end of the acute phase to the end of the 3-year follow-up period ('long-term phase').
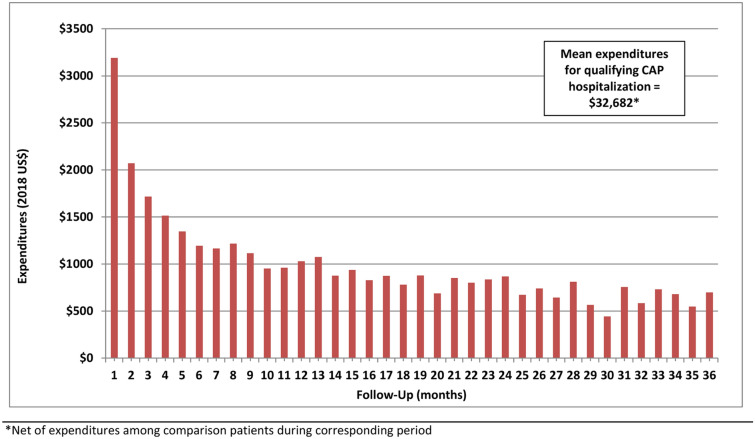
The study population included 43,975 matched pairs of CAP patients and comparison patients. Expenditures averaged $33,380 (95% confidence interval [CI] $32,665-$34,161) for the CAP hospitalization and $4568 (95% CI $4385-$4749) during the 30-day period thereafter (vs. $2075 [95% CI $1989-$2167] in total for the comparison patients). During the long-term phase, all-cause expenditures averaged $83,463 (95% CI $81,318-$85,784) for CAP patients versus $51,017 (95% CI $49,553-$52,491) for comparison patients, and thus attributable expenditures during this phase totaled $32,446 (95% CI $29,847-$35,075). The majority of attributable CAP expenditures (53% of $68,319) occurred during the acute phase, while 21%, 14%, and 12% occurred during the first, second, and third years, respectively, after the acute phase.
Our findings provide additional evidence that the cost of CAP requiring hospitalization is high, and that the impact of CAP extends well beyond the expected time for resolution of acute inflammatory signs.
虽然人们对社区获得性肺炎(CAP)急性期的费用了解很多,但对其后潜在的可归因费用却知之甚少。
本研究的目的是评估美国临床实践中成年人CAP相关的长期可归因费用。
采用回顾性匹配队列设计和来自美国私人医疗保健索赔库的数据。在研究期间(2011 - 2016年)的每个月,当月因CAP住院的成年人(“CAP患者”)在人口统计学、临床和医疗保健概况方面与当月未发生CAP的成年人(“对照患者”)进行匹配(1:1,无替换)。统计符合条件的CAP住院期间以及出院后30天内(统称为“急性期”)的全因医疗保健支出,以及从急性期结束到3年随访期结束(“长期期”)的支出。
研究人群包括43,975对匹配的CAP患者和对照患者。CAP住院期间的支出平均为33,380美元(95%置信区间[CI] 32,665 - 34,161美元),此后30天内平均为4568美元(95% CI 4385 - 4749美元)(对照患者总计为2075美元[95% CI 1989 - 2167美元])。在长期期,CAP患者的全因支出平均为83,463美元(95% CI 81,318 - 85,784美元),对照患者为51,017美元(95% CI 49,553 - 52,491美元),因此该阶段的可归因支出总计为32,446美元(95% CI 29,847 - 35,075美元)。大多数可归因于CAP的支出(占68,319美元的53%)发生在急性期,而分别在急性期后的第一年、第二年和第三年发生的占21%、14%和12%。
我们的研究结果提供了更多证据,表明需要住院治疗的CAP费用很高,而且CAP的影响远远超出急性炎症体征消退的预期时间。