Department of Anesthesia, Critical Care and Emergency, Fondazione IRCCS Ca' Granda Ospedale Maggiore Policlinico, Milan, Italy.
Department of Pathophysiology and Transplantation, University of Milan, Via F. Sforza 35, 20122, Milan, Italy.
Crit Care. 2020 Nov 23;24(1):654. doi: 10.1186/s13054-020-03344-0.
Nasal high flow delivered at flow rates higher than 60 L/min in patients with acute hypoxemic respiratory failure might be associated with improved physiological effects. However, poor comfort might limit feasibility of its clinical use.
We performed a prospective randomized cross-over physiological study on 12 ICU patients with acute hypoxemic respiratory failure. Patients underwent three steps at the following gas flow: 0.5 L/kg PBW/min, 1 L/kg PBW/min, and 1.5 L/kg PBW/min in random order for 20 min. Temperature and FiO remained unchanged. Toward the end of each phase, we collected arterial blood gases, lung volumes, and regional distribution of ventilation assessed by electrical impedance tomography (EIT), and comfort.
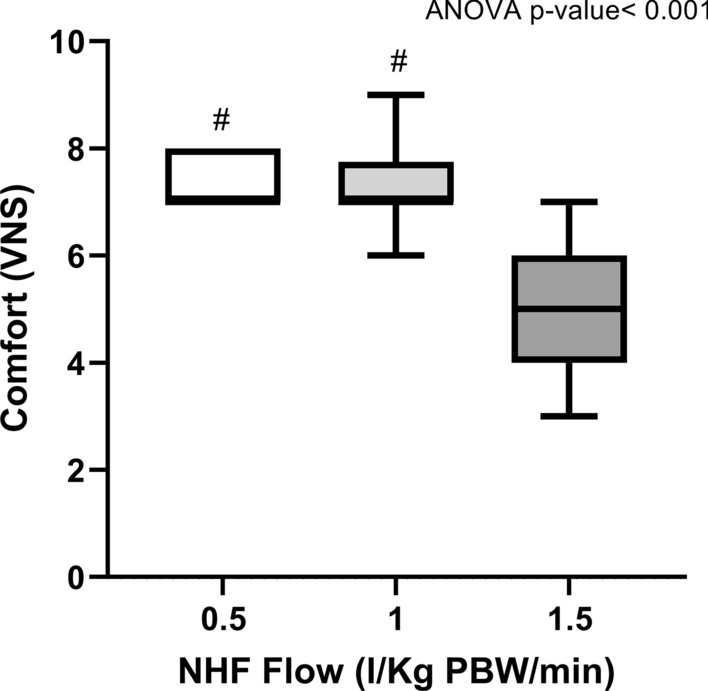
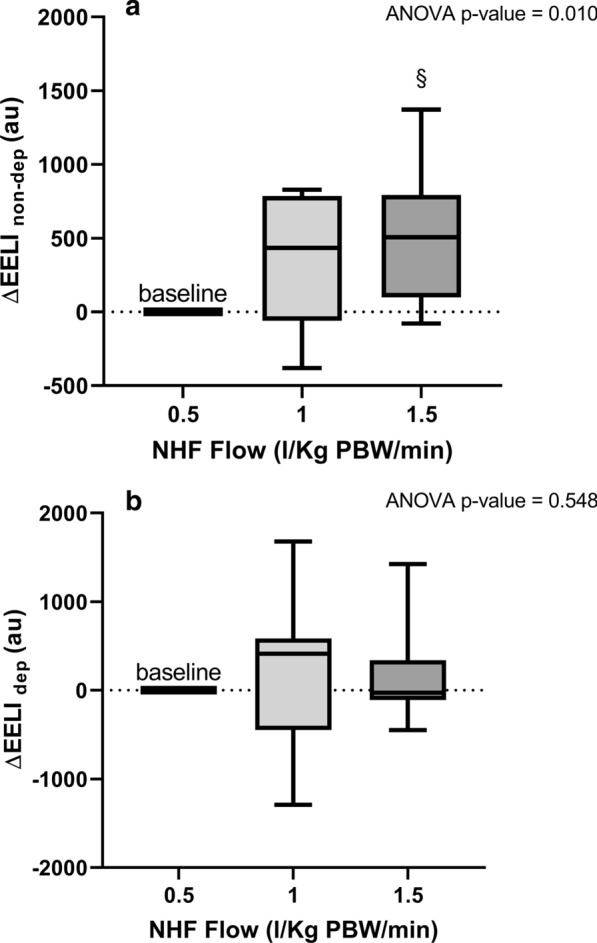
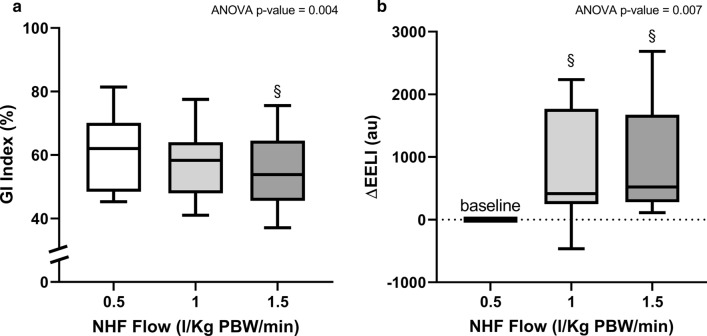
In five patients, the etiology was pulmonary; infective disease characterized seven patients; median PaO/FiO at enrollment was 213 [IQR 136-232]. The range of flow rate during NHF 1.5 was 75-120 L/min. PaO/FiO increased with flow, albeit non significantly (p = 0.064), PaCO and arterial pH remained stable (p = 0.108 and p = 0.105). Respiratory rate decreased at higher flow rates (p = 0.014). Inhomogeneity of ventilation decreased significantly at higher flows (p = 0.004) and lung volume at end-expiration significantly increased (p = 0.007), but mostly in the non-dependent regions. Comfort was significantly poorer during the step performed at the highest flow (p < 0.001).
NHF delivered at rates higher than 60 L/min in critically ill patients with acute hypoxemic respiratory failure is associated with reduced respiratory rate, increased lung homogeneity, and additional positive pressure effect, but also with worse comfort.
在急性低氧性呼吸衰竭患者中,以高于 60L/min 的流速输送鼻高流量可能与改善生理效应有关。然而,较差的舒适度可能会限制其临床应用的可行性。
我们对 12 例急性低氧性呼吸衰竭的 ICU 患者进行了前瞻性随机交叉生理研究。患者以随机顺序在以下气体流速下进行三步:0.5L/kgPBW/min、1L/kgPBW/min 和 1.5L/kgPBW/min,持续 20min。温度和 FiO 保持不变。在每个阶段结束时,我们采集动脉血气、肺容积以及通过电阻抗断层成像(EIT)评估的通气区域分布,并评估舒适度。
在五名患者中,病因是肺部;感染性疾病特征为七名患者;入组时的 PaO/FiO 中位数为 213[IQR 136-232]。NHF1.5 期间的流量范围为 75-120L/min。尽管非显著性(p=0.064),但随着流量增加 PaO/FiO 增加,PaCO 和动脉 pH 保持稳定(p=0.108 和 p=0.105)。随着流速增加,呼吸频率降低(p=0.014)。在更高的流速下,通气不均匀性显著降低(p=0.004),呼气末期肺容积显著增加(p=0.007),但主要在非依赖区。在最高流速下进行的步骤中,舒适度显著较差(p<0.001)。
在急性低氧性呼吸衰竭的危重症患者中,以高于 60L/min 的流速输送鼻高流量与降低呼吸频率、增加肺均匀性和附加正压效应有关,但舒适度也较差。