Department of Clinical Science, Intervention and Technology (CLINTEC), Karolinska Institutet, Stockholm, Sweden.
Department of Surgery, Södersjukhuset, Stockholm, Sweden.
Langenbecks Arch Surg. 2021 Aug;406(5):1415-1423. doi: 10.1007/s00423-020-02037-0. Epub 2020 Nov 24.
Insertion of a nutritional jejunostomy in conjunction with esophagectomy is performed with the intention to decrease the risk for postoperative malnutrition and improve recovery without adding significant catheter-related complications. However, previous research has shown no clear benefit and there is currently no consensus of practice.
All patients treated with esophagectomy due to cancer during the period 2006-2017 reported in the Swedish National Register for Esophageal and Gastric Cancer were included in this register-based cohort study from a national database. Patients were stratified into two groups: esophagectomy alone and esophagectomy with jejunostomy.
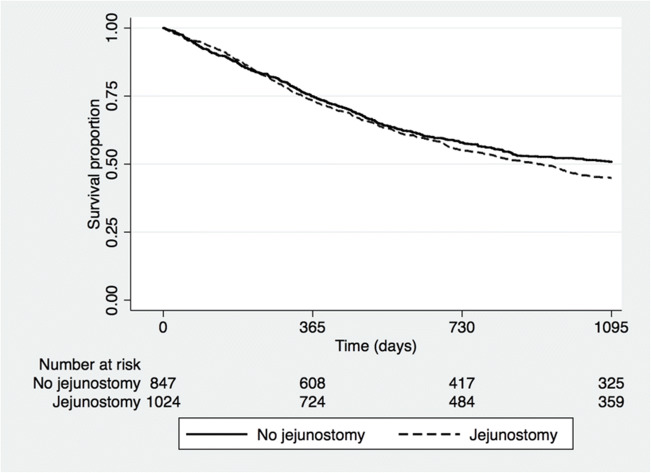
A total of 847 patients (45.27%) had no jejunostomy inserted while 1024 patients (54.73%) were treated with jejunostomy. The groups were comparable, but some differences were seen in histological tumor type and tumor stage between the groups. No significant differences in length of hospital stay, postoperative surgical complications, Clavien-Dindo score, or 90-day mortality rate were seen. There was no evidence of increased risk for significant jejunostomy-related complications. Patients in the jejunostomy group with anastomotic leaks had a statistically significant lower risk for severe morbidity defined as Clavien-Dindo score ≥ IIIb (adjusted odds ratio 0.19, 95% CI: 0.04-0.94, P = 0.041) compared to patients with anastomotic leaks and no jejunostomy.
A nutritional jejunostomy is a safe method for early postoperative enteral nutrition which might decrease the risk for severe outcomes in patients with anastomotic leaks. Nutritional jejunostomy should be considered for patients undergoing curative intended surgery for esophageal and gastro-esophageal junction cancer.
在食管癌切除术中插入营养性空肠造口术的目的是降低术后营养不良的风险,促进恢复,而不会增加显著的导管相关并发症。然而,先前的研究并未显示出明显的益处,目前也没有达成实践共识。
本研究基于国家数据库,对 2006 年至 2017 年间在瑞典食管癌和胃癌登记处报告的所有接受食管癌切除术治疗的癌症患者进行了回顾性队列研究。患者分为两组:单纯食管癌切除术组和食管癌切除术加空肠造口术组。
共 847 例(45.27%)患者未插入空肠造口,1024 例(54.73%)患者接受了空肠造口术。两组患者在组织学肿瘤类型和肿瘤分期方面具有可比性,但存在一些差异。两组患者的住院时间、术后手术并发症、Clavien-Dindo 评分或 90 天死亡率均无显著差异。空肠造口术相关并发症的风险也没有增加的证据。空肠造口术组吻合口漏的患者发生严重并发症(定义为 Clavien-Dindo 评分≥IIIb)的风险显著降低(调整比值比 0.19,95%CI:0.04-0.94,P=0.041),与无空肠造口术组吻合口漏患者相比。
营养性空肠造口术是一种安全的术后早期肠内营养方法,可能降低吻合口漏患者发生严重结局的风险。对于接受根治性手术治疗的食管和胃食管交界部癌症患者,应考虑使用空肠造口术。