Curtius Kit, Rubenstein Joel H, Chak Amitabh, Inadomi John M
Centre for Genomics and Computational Biology, Barts Cancer Institute, School of Medicine and Dentistry, Queen Mary University of London, London, UK
Division of Biomedical Informatics, Department of Medicine, University of California San Diego, La Jolla, California, USA.
Gut. 2020 Nov 24;70(8):1435-40. doi: 10.1136/gutjnl-2020-321598.
Barrett's oesophagus (BE) is a known precursor to oesophageal adenocarcinoma (OAC) but current clinical data have not been consolidated to address whether BE is the origin of all incident OAC, which would reinforce evidence for BE screening efforts. We aimed to answer whether all expected prevalent BE, diagnosed and undiagnosed, could account for all incident OACs in the US cancer registry data.
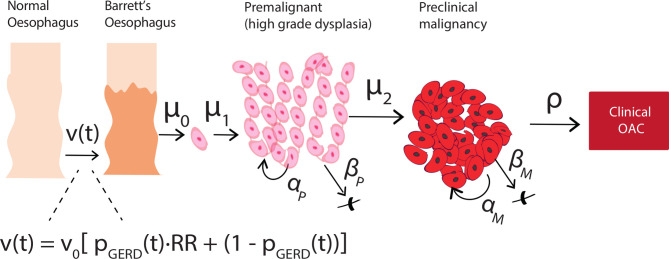
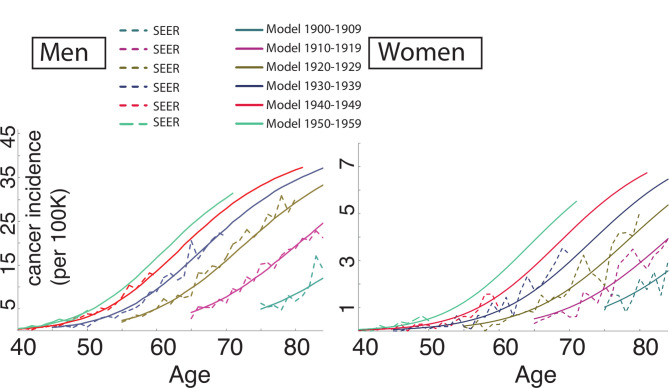
We used a multiscale computational model of OAC that includes the evolutionary process from normal oesophagus through BE in individuals from the US population. The model was previously calibrated to fit Surveillance, Epidemiology and End Results cancer incidence curves. Here, we also utilised age-specific and sex-specific US census data for numbers at-risk. The primary outcome for model validation was the expected number of OAC cases for a given calendar year. Secondary outcomes included the comparisons of resulting model-predicted prevalence of BE and BE-to-OAC progression to the observed prevalence and progression rates.
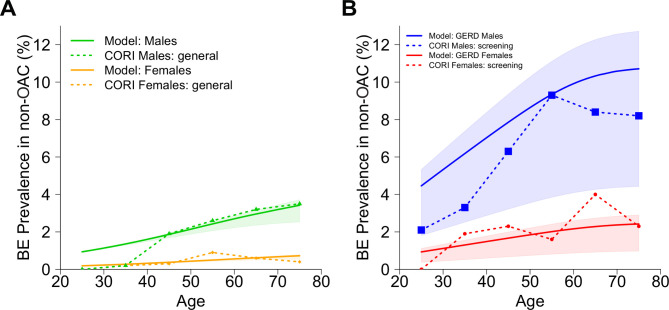
The model estimated the total number of OAC cases from BE in 2010 was 9970 (95% CI: 9140 to 11 980), which recapitulates nearly all OAC cases from population data. The model simultaneously predicted 8%-9% BE prevalence in high-risk males age 45-55, and 0.1%-0.2% non-dysplastic BE-to-OAC annual progression in males, consistent with clinical studies.
There are likely few additional OAC cases arising in the US population outside those expected from individuals with BE. Effective screening of high-risk patients could capture the majority of population destined for OAC progression and potentially decrease mortality through early detection and curative removal of small (pre)cancers during surveillance.
巴雷特食管(BE)是食管腺癌(OAC)已知的癌前病变,但目前的临床数据尚未整合,以解决BE是否是所有新发OAC的起源,这将加强BE筛查工作的证据。我们旨在回答在美国癌症登记数据中,所有预期的已诊断和未诊断的BE病例是否能解释所有新发OAC病例。
我们使用了一个OAC的多尺度计算模型,该模型包括美国人群中个体从正常食管通过BE的演变过程。该模型先前已校准以拟合监测、流行病学和最终结果癌症发病率曲线。在这里,我们还利用了按年龄和性别分类的美国人口普查数据来计算风险人数。模型验证的主要结果是给定日历年度的OAC病例预期数量。次要结果包括将模型预测的BE患病率和BE向OAC进展率与观察到的患病率和进展率进行比较。
该模型估计2010年由BE导致的OAC病例总数为9970例(95%CI:9140至11980),这几乎概括了人群数据中的所有OAC病例。该模型同时预测,45 - 55岁高危男性中BE患病率为8% - 9%,男性中无发育异常的BE向OAC的年进展率为0.1% - 0.2%,与临床研究一致。
在美国人群中,除了那些预计由BE患者产生的OAC病例外,可能几乎没有其他OAC病例。对高危患者进行有效筛查可以捕获大多数有OAC进展风险的人群,并有可能通过在监测期间早期发现和根治性切除小(前)癌来降低死亡率。