Snyder Kristi K, Van Buskirk Robert G, Baust John G, Baust John M
CPSI Biotech, Owego, NY, USA.
Center for Translational Stem Cell and Tissue Engineering, Binghamton University, Binghamton, NY, USA.
Breast Cancer (Auckl). 2020 Nov 12;14:1178223420972363. doi: 10.1177/1178223420972363. eCollection 2020.
Breast cancer is the most prominent form of cancer and the second leading cause of death in women behind lung cancer. The primary modes of treatment today include surgical excision (lumpectomy, mastectomy), radiation, chemoablation, anti-HER2/neu therapy, and/or hormone therapy. The severe side effects associated with these therapies suggest a minimally invasive therapy with fewer quality of life issues would be advantageous for treatment of this pervasive disease. Cryoablation has been used in the treatment of other cancers, including prostate, skin, and cervical, for decades and has been shown to be a successful minimally invasive therapeutic option. To this end, the use of cryotherapy for the treatment of breast cancer has increased over the last several years. Although successful, one of the challenges in cryoablation is management of cancer destruction in the periphery of the ice ball as the tissue within this outer margin may not experience ablative temperatures. In breast cancer, this is of concern due to the lobular nature of the tumors. As such, in this study, we investigated the level of cell death at various temperatures associated with the margin of a cryogenic lesion as well as the impact of repetitive freezing and thawing methods on overall efficacy.
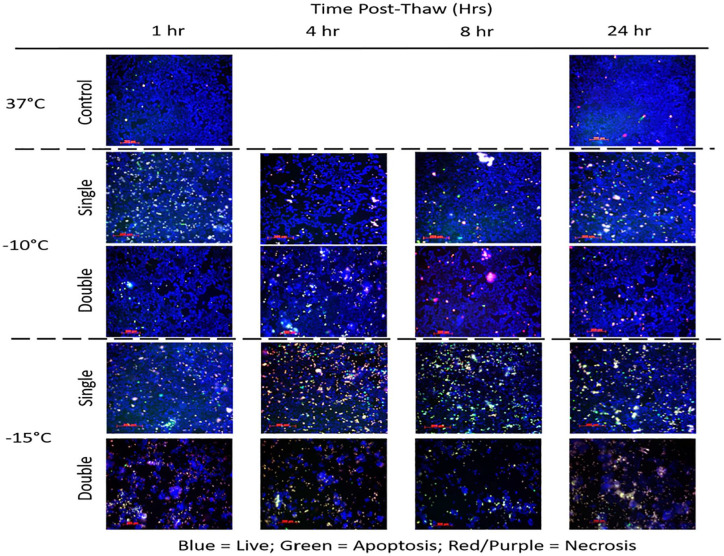
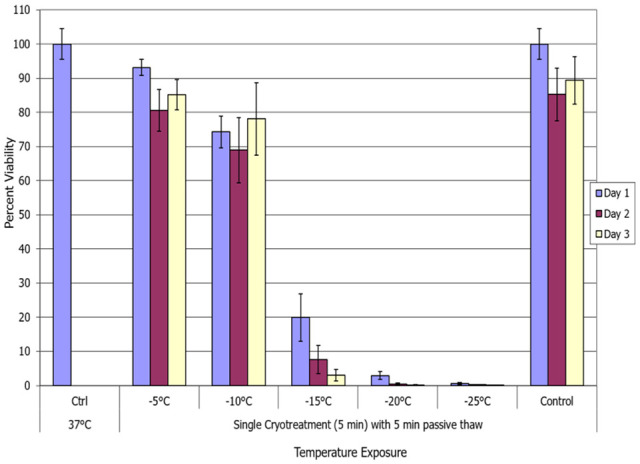
Human breast cancer cells, MCF-7, were exposed to temperatures of -5°C, -10°C, -15°C, -20°C, or -25°C for 5-minute freeze intervals in a single or repeat freeze-thaw cycle. Samples were thawed with either passive or active warming for 5 or 10 minutes. Samples were assessed at 1, 2, and 3 days post-freeze to assess cell survival and recovery. In addition, the modes of cell death associated with freezing were assessed over the initial 24-hour post-thaw recovery period.
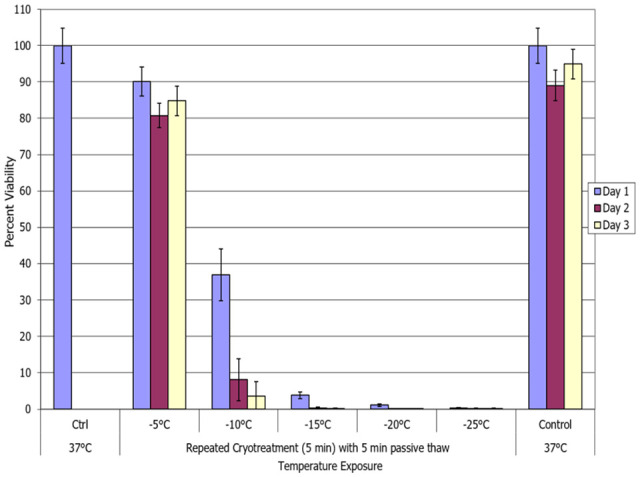
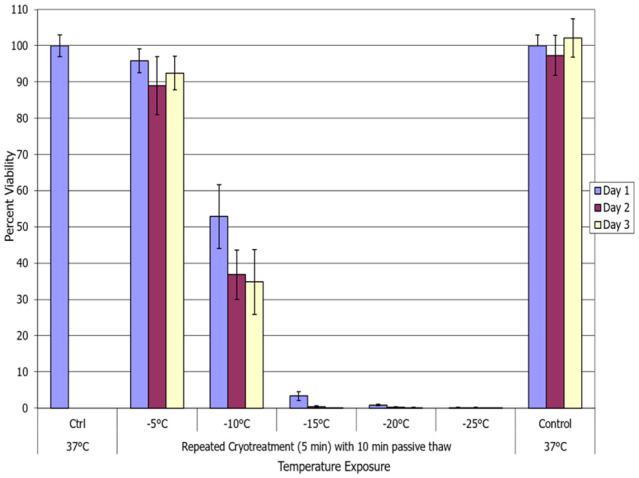
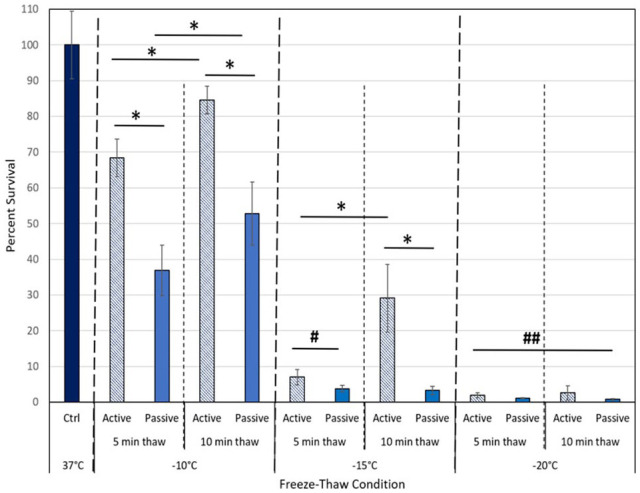
Exposure of MCF-7 cells to -5°C and -10°C resulted in minimal cell death regardless of the freeze/thaw conditions. Freezing to a temperature of -25°C resulted in complete cell death 1 day post-thaw with no cell recovery in all freeze/thaw scenarios evaluated. Exposure to a single freeze event resulted in a gradual increase in cell death at -15°C and -20°C. Application of a repeat freeze-thaw cycle (dual 5-minute freeze) resulted in an increase in cell death with complete destruction at -20°C and near complete death at -15°C (day 1 survival: single -15°C freeze/thaw = 20%; repeated -15°C freeze/thaw = 4%). Analysis of thaw interval time (5 vs 10 minute) demonstrated that the shorter 5-minute thaw interval between freezes resulted in increased cell destruction. Furthermore, investigation of thaw rate (active vs passive thawing) demonstrated that active thawing resulted in increased cell survival thereby less effective ablation compared with passive thawing (eg, -15°C 5/10/5 procedure survival, passive thaw: 4% vs active thaw: 29%).
In summary, these in vitro findings suggest that freezing to temperatures of 25°C results in a high degree of breast cancer cell destruction. Furthermore, the data demonstrate that the application of a repeat freeze procedure with a passive 5-minute or 10-minute thaw interval between freeze cycles increases the minimal lethal temperature to the -15°C to -20°C range. The data also demonstrate that the use of an active thawing procedure between freezes reduces ablation efficacy at temperatures associated with the iceball periphery. These findings may be important to improving future clinical applications of cryoablation for the treatment of breast cancer.
乳腺癌是最常见的癌症形式,也是女性仅次于肺癌的第二大死因。目前的主要治疗方式包括手术切除(乳房肿瘤切除术、乳房切除术)、放疗、化学消融、抗HER2/neu治疗和/或激素治疗。这些治疗方法所带来的严重副作用表明,一种对生活质量影响较小的微创治疗方法对于治疗这种普遍存在的疾病将是有利的。冷冻消融已用于治疗其他癌症,包括前列腺癌、皮肤癌和宫颈癌,已有数十年历史,并且已被证明是一种成功的微创治疗选择。为此,在过去几年中,使用冷冻疗法治疗乳腺癌的情况有所增加。尽管取得了成功,但冷冻消融的挑战之一是处理冰球边缘的癌症破坏情况,因为该外缘内的组织可能未经历消融温度。在乳腺癌中,由于肿瘤的小叶性质,这一点令人担忧。因此,在本研究中,我们调查了与低温损伤边缘相关的不同温度下的细胞死亡水平,以及重复冻融方法对整体疗效的影响。
将人乳腺癌细胞MCF-7在-5°C、-10°C、-15°C、-20°C或-25°C的温度下暴露5分钟的冷冻间隔时间,进行单次或重复冻融循环。样品通过被动或主动复温解冻5或10分钟。在冷冻后1、2和3天对样品进行评估,以评估细胞存活和恢复情况。此外,在解冻后最初的24小时恢复期内评估与冷冻相关的细胞死亡模式。
无论冻融条件如何,将MCF-7细胞暴露于-5°C和-10°C导致的细胞死亡极少。冷冻至-25°C的温度导致解冻后1天细胞完全死亡,在所评估的所有冻融情况下均无细胞恢复。单次冷冻事件导致在-15°C和-20°C时细胞死亡逐渐增加。应用重复冻融循环(两次5分钟冷冻)导致细胞死亡增加,在-20°C时完全破坏,在-15°C时接近完全死亡(第1天存活率:单次-15°C冻融=20%;重复-15°C冻融=4%)。对解冻间隔时间(5分钟与10分钟)的分析表明,两次冷冻之间较短的5分钟解冻间隔导致细胞破坏增加。此外,对解冻速率(主动与被动解冻)的研究表明,与被动解冻相比,主动解冻导致细胞存活率增加,从而消融效果较差(例如,-15°C 5/10/5程序存活率,被动解冻:4%对主动解冻:29%)。
总之,这些体外研究结果表明,冷冻至25°C的温度会导致高度的乳腺癌细胞破坏。此外,数据表明,在冷冻循环之间应用被动5分钟或10分钟解冻间隔的重复冷冻程序会将最低致死温度提高到-15°C至-20°C范围。数据还表明,在冷冻之间使用主动解冻程序会降低与冰球边缘相关温度下的消融效果。这些发现可能对改善未来冷冻消融治疗乳腺癌的临床应用很重要。