Baust John M, Robilotto Anthony, Snyder Kristi K, Santucci Kimberly, Stewart Jennie, Van Buskirk Robert, Baust John G
CPSI Biotect, Owego, NY, USA.
Institute of Biomedical Technology, Binghamton University, Binghamton, NY, USA.
Technol Cancer Res Treat. 2017 Dec;16(6):900-909. doi: 10.1177/1533034617708960. Epub 2017 May 17.
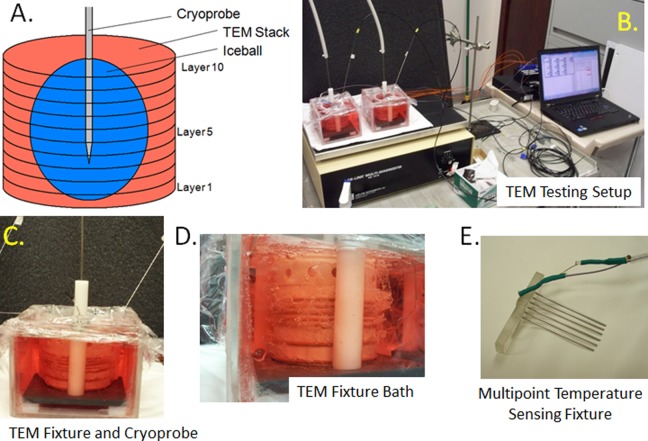
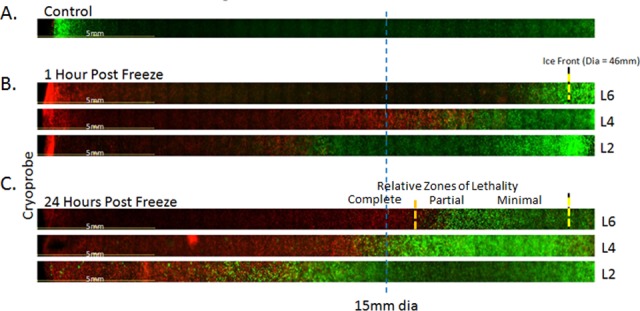
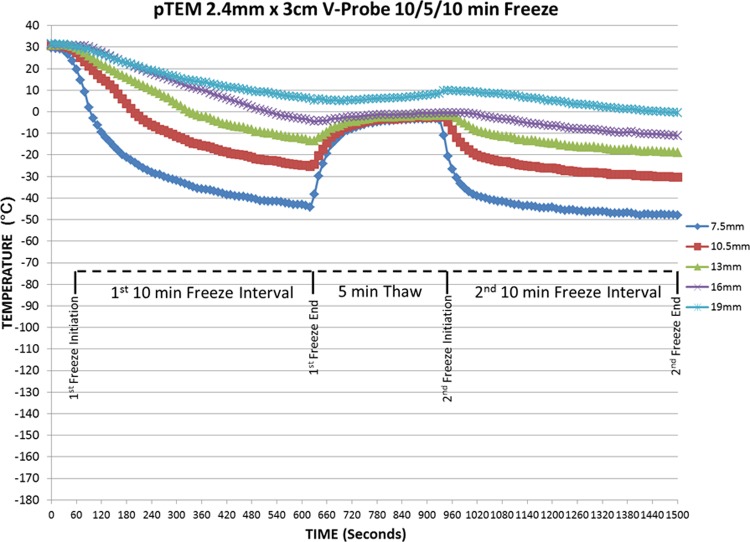
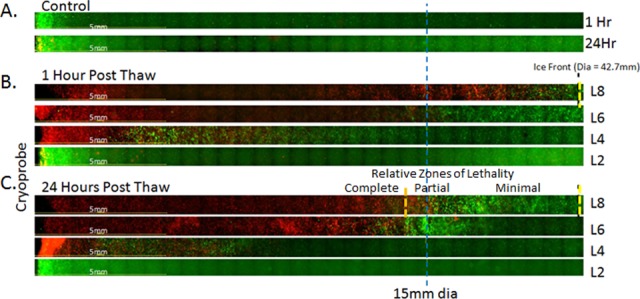
As the clinical use of cryoablation for the treatment of cancer has increased, so too has the need for knowledge on the dynamic environment within the frozen mass created by a cryoprobe. While a number of factors exist, an understanding of the iceball size, critical isotherm distribution/penetration, and the resultant lethal zone created by a cryoprobe are critical for clinical application. To this end, cryoprobe performance is typically characterized based on the iceball size and temperature penetration in phantom gel models. Although informative, these models do not provide information as to the impact of heat input from surrounding tissue nor give any information on the ablative zone created. As such, we evaluated the use of a tissue-engineered tumor model (TEM) to assess cryoprobe performance including iceball size, real-time thermal profile distribution, and resultant ablative zone. Studies were conducted using an Endocare V-probe cryoprobe, with a 10/5/10 double freeze-thaw protocol using prostate and renal cancer TEMs. The data demonstrate the generation of a 33- to 38-cm3 frozen mass with the V-Probe cryoprobe following the double freeze of which ∼12.7 and 6.5 cm3 was at or below -20°C and -40°C, respectively. Analysis of ablation zone using fluorescence microscopy 24 hours postthaw demonstrated that the internal ∼40% of the frozen mass was completely ablated, whereas in the periphery of the iceball (outer 1 cm region), a gradient of partial to minimal destruction was observed. These findings correlated well with clinical reports on renal and prostate cancer cryoablation. Overall, this study demonstrates that TEMs provide an effective model for a more complete characterization of cryoablation device performance. The data demonstrate that while the overall iceball size generated in the TEM was consistent with published reports from phantom models, the integration of an external heat load, circulation, and cellular components more closely reflect an setting and the impact of penetration of the critical (-20°C and -40°C) isotherms into the tissue. This is important as it is well appreciated in clinical practice that the heat load of a tissue, cryoprobe proximity to vasculature, and so on, can impact outcome. The TEM model provides a means of characterizing the impact on ablative dose delivery allowing for a better understanding of probe performance and potential impact on ablative outcome.
随着冷冻消融技术在癌症治疗中的临床应用不断增加,对于了解冷冻探针所形成的冷冻组织块内动态环境的需求也日益增长。虽然存在多种因素,但了解冰球大小、临界等温线分布/穿透情况以及冷冻探针所形成的致死区对于临床应用至关重要。为此,冷冻探针的性能通常基于其在模拟凝胶模型中的冰球大小和温度穿透情况来表征。尽管这些模型提供了一定信息,但它们并未提供关于周围组织热输入影响的信息,也未给出任何关于所形成消融区的信息。因此,我们评估了使用组织工程肿瘤模型(TEM)来评估冷冻探针的性能,包括冰球大小、实时热分布图以及所形成的消融区。研究使用Endocare V型探针冷冻探针,采用10/5/10双冻融方案,使用前列腺癌和肾癌TEM模型。数据表明,在双冻后,V型探针冷冻探针可形成33至38立方厘米的冷冻组织块,其中分别约有12.7立方厘米和6.5立方厘米处于或低于-20°C和-40°C。解冻后24小时使用荧光显微镜对消融区进行分析表明,冷冻组织块内部约40%被完全消融,而在冰球周边(外侧1厘米区域),观察到从部分破坏到最小破坏的梯度变化。这些发现与关于肾癌和前列腺癌冷冻消融的临床报告高度相关。总体而言,本研究表明TEM模型为更全面地表征冷冻消融设备性能提供了一个有效模型。数据表明,虽然TEM模型中所形成的总体冰球大小与模拟模型的已发表报告一致,但外部热负荷、循环和细胞成分的整合更紧密地反映了实际情况以及临界(-20°C和-40°C)等温线向组织内的穿透影响。这一点很重要,因为在临床实践中人们清楚地认识到组织的热负荷、冷冻探针与血管的接近程度等会影响治疗结果。TEM模型提供了一种表征对消融剂量传递影响的方法,有助于更好地理解探针性能以及对消融结果的潜在影响。