Hospital Infantil Universitario Niño Jesús, Madrid, Spain.
Hospital Universitario Son Espases, Palma, Spain.
Crit Care. 2020 Nov 26;24(1):666. doi: 10.1186/s13054-020-03332-4.
Multisystem inflammatory syndrome temporally associated with COVID-19 (MIS-C) has been described as a novel and often severe presentation of SARS-CoV-2 infection in children. We aimed to describe the characteristics of children admitted to Pediatric Intensive Care Units (PICUs) presenting with MIS-C in comparison with those admitted with SARS-CoV-2 infection with other features such as COVID-19 pneumonia.
A multicentric prospective national registry including 47 PICUs was carried out. Data from children admitted with confirmed SARS-CoV-2 infection or fulfilling MIS-C criteria (with or without SARS-CoV-2 PCR confirmation) were collected. Clinical, laboratory and therapeutic features between MIS-C and non-MIS-C patients were compared.
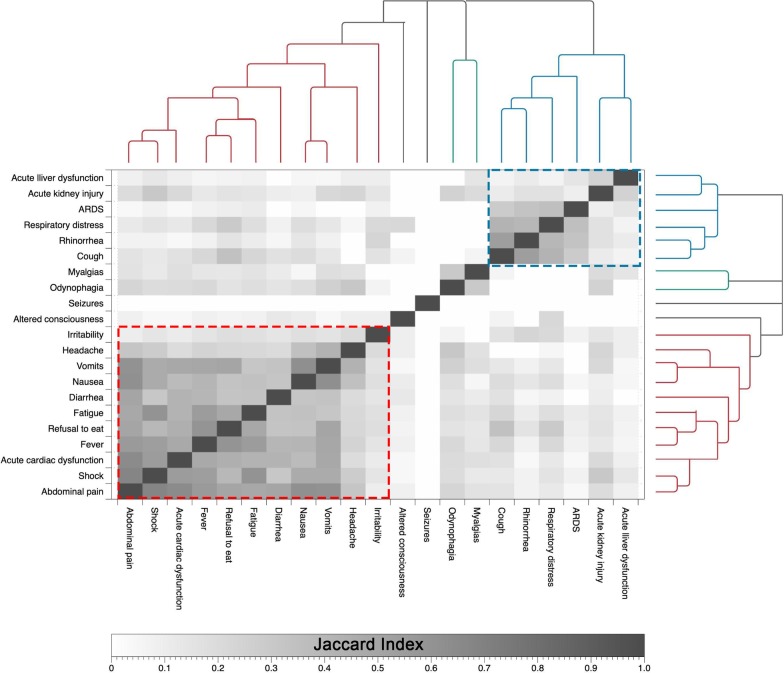
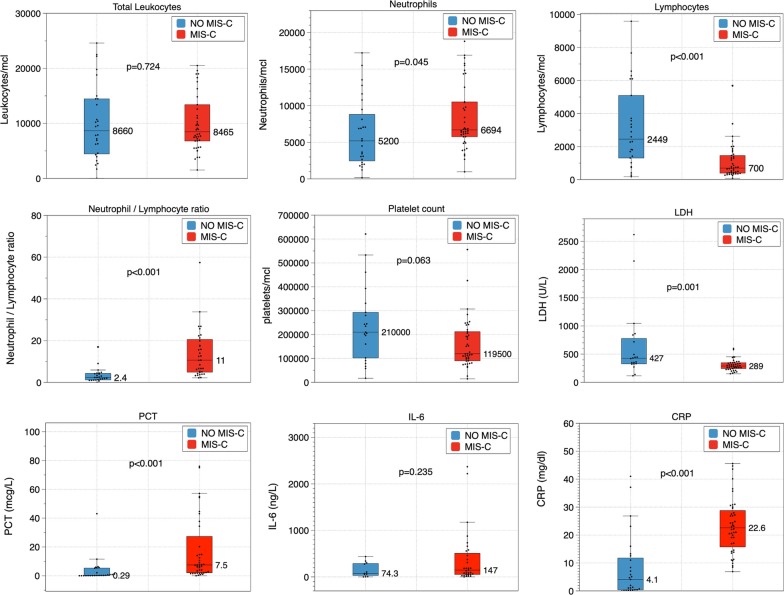
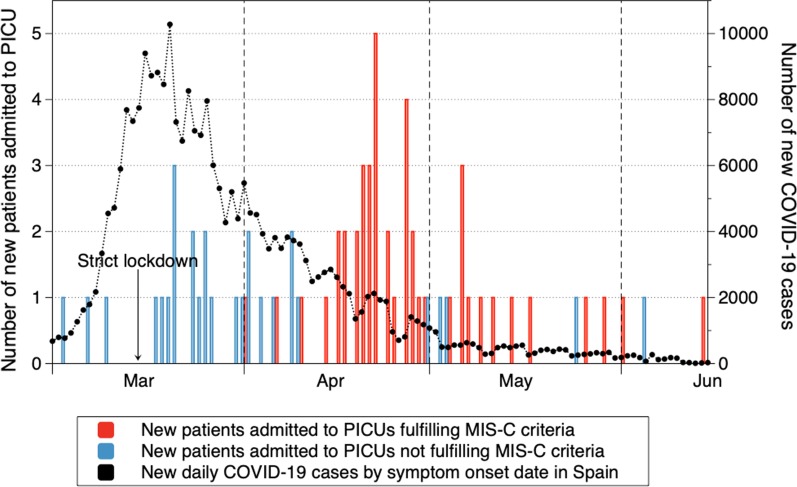
Seventy-four children were recruited. Sixty-one percent met MIS-C definition. MIS-C patients were older than non-MIS-C patients (p = 0.002): 9.4 years (IQR 5.5-11.8) vs 3.4 years (IQR 0.4-9.4). A higher proportion of them had no previous medical history of interest (88.2% vs 51.7%, p = 0.005). Non-MIS-C patients presented more frequently with respiratory distress (60.7% vs 13.3%, p < 0.001). MIS-C patients showed higher prevalence of fever (95.6% vs 64.3%, p < 0.001), diarrhea (66.7% vs 11.5%, p < 0.001), vomits (71.1% vs 23.1%, p = 0.001), fatigue (65.9% vs 36%, p = 0.016), shock (84.4% vs 13.8%, p < 0.001) and cardiac dysfunction (53.3% vs 10.3%, p = 0.001). MIS-C group had a lower lymphocyte count (p < 0.001) and LDH (p = 0.001) but higher neutrophil count (p = 0.045), neutrophil/lymphocyte ratio (p < 0.001), C-reactive protein (p < 0.001) and procalcitonin (p < 0.001). Patients in the MIS-C group were less likely to receive invasive ventilation (13.3% vs 41.4%, p = 0.005) but were more often treated with vasoactive drugs (66.7% vs 24.1%, p < 0.001), corticosteroids (80% vs 44.8%, p = 0.003) and immunoglobulins (51.1% vs 6.9%, p < 0.001). Most patients were discharged from PICU by the end of data collection with a median length of stay of 5 days (IQR 2.5-8 days) in the MIS-C group. Three patients died, none of them belonged to the MIS-C group.
MIS-C seems to be the most frequent presentation among critically ill children with SARS-CoV-2 infection. MIS-C patients are older and usually healthy. They show a higher prevalence of gastrointestinal symptoms and shock and are more likely to receive vasoactive drugs and immunomodulators and less likely to need mechanical ventilation than non-MIS-C patients.
与 COVID-19 相关的儿童多系统炎症综合征(MIS-C)已被描述为 SARS-CoV-2 感染的一种新的且通常较为严重的表现。本研究旨在描述与其他 SARS-CoV-2 感染特征(如 COVID-19 肺炎)相比,因 MIS-C 而入住儿科重症监护病房(PICU)的儿童的特征。
进行了一项多中心前瞻性全国性登记研究,共纳入了 47 家 PICU。收集了确诊 SARS-CoV-2 感染或符合 MIS-C 标准(无论是否有 SARS-CoV-2 PCR 确认)的儿童的数据。比较了 MIS-C 与非 MIS-C 患者的临床、实验室和治疗特征。
共纳入 74 例患儿。61%的患儿符合 MIS-C 定义。MIS-C 患儿较非 MIS-C 患儿年龄更大(p=0.002):9.4 岁(IQR 5.5-11.8)vs 3.4 岁(IQR 0.4-9.4)。无其他相关既往病史的患儿比例更高(88.2% vs 51.7%,p=0.005)。非 MIS-C 患儿更常出现呼吸窘迫(60.7% vs 13.3%,p<0.001)。MIS-C 患儿发热(95.6% vs 64.3%,p<0.001)、腹泻(66.7% vs 11.5%,p<0.001)、呕吐(71.1% vs 23.1%,p=0.001)、乏力(65.9% vs 36%,p=0.016)、休克(84.4% vs 13.8%,p<0.001)和心功能障碍(53.3% vs 10.3%,p=0.001)更为常见。MIS-C 组患儿的淋巴细胞计数(p<0.001)和乳酸脱氢酶(p=0.001)更低,但中性粒细胞计数(p=0.045)、中性粒细胞/淋巴细胞比值(p<0.001)、C 反应蛋白(p<0.001)和降钙素原(p<0.001)更高。MIS-C 组患儿接受有创通气的可能性更小(13.3% vs 41.4%,p=0.005),但接受血管活性药物(66.7% vs 24.1%,p<0.001)、皮质类固醇(80% vs 44.8%,p=0.003)和免疫球蛋白(51.1% vs 6.9%,p<0.001)治疗的可能性更高。大多数患儿在数据收集结束时从 PICU出院,MIS-C 组患儿的中位住院时间为 5 天(IQR 2.5-8 天)。3 例患儿死亡,均不属于 MIS-C 组。
MIS-C 似乎是 SARS-CoV-2 感染危重症患儿最常见的表现。MIS-C 患儿年龄较大且通常健康。与非 MIS-C 患儿相比,MIS-C 患儿胃肠道症状和休克更为常见,更可能接受血管活性药物和免疫调节剂治疗,而不太可能需要机械通气。