Liu Yi-Chi, Chang Hung-Ming, Lin Hsin-Hon, Lu Chia-Chun, Lai Lu-Han
Institute of Nuclear Engineering and Science, National Tsing Hua University, Hsinchu 30015 Taiwan.
Department of Radiation Oncology, Wei Gong Memorial Hospital, Miaoli 35148, Taiwan.
J Clin Med. 2020 Nov 29;9(12):3884. doi: 10.3390/jcm9123884.
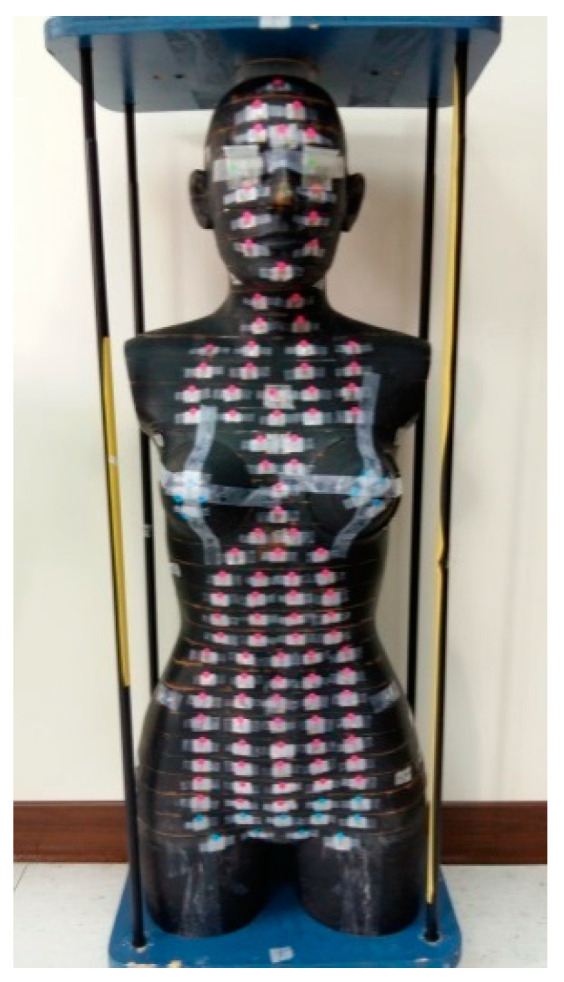
This study aimed to compare different types of right breast cancer radiotherapy planning techniques and to estimate the whole-body effective doses and the critical organ absorbed doses. The three planning techniques are intensity-modulated radiotherapy (IMRT), volumetric modulated arc therapy (VMAT; two methods) and hybrid 3D-CRT/IMRT (three-dimensional conformal radiotherapy/intensity-modulated radiotherapy). The VMAT technique includes two methods to deliver a dose: non-continuous partial arc and continuous partial arc. A thermoluminescent dosimeter (TLD) is placed in the RANDO phantom to estimate the organ absorbed dose. Each planning technique applies 50.4 Gy prescription dose and treats critical organs, including the lung and heart. Dose-volume histogram was used to show the planning target volume (V95%), homogeneity index (HI), conformity index (CI), and other optimized indices. The estimation of whole-body effective dose was based on the International Commission on Radiation Protection (ICRP) Publication 60 and 103. The results were as follows: Continuous partial arc and non-continuous partial arc showed the best CI and HI. The heart absorbed doses in the continuous partial arc and hybrid 3D-CRT/IMRT were 0.07 ± 0.01% and 0% (V5% and V10%, respectively). The mean dose of the heart was lowest in hybrid 3D-CRT/IMRT (1.47 Gy ± 0.02). The dose in the left contralateral lung (V5%) was lowest in continuous partial arc (0%). The right ipsilateral lung average dose and V20% are lowest in continuous partial arc. Hybrid 3D-CRT/IMRT has the lowest mean dose to contralateral breast (organs at risk). The whole-body effective doses for ICRP-60 and ICRP-103 were highest in continuous partial arc (2.01 Sv ± 0.23 and 2.89 Sv ± 0.15, respectively). In conclusion, the use of VMAT with continuous arc has a lower risk of radiation pneumonia, while hybrid 3D-CRT/IMRT attain lower secondary malignancy risk and cardiovascular complications.
本研究旨在比较不同类型的右乳腺癌放射治疗计划技术,并估算全身有效剂量和关键器官吸收剂量。三种计划技术分别是调强放射治疗(IMRT)、容积调强弧形治疗(VMAT;两种方法)和混合3D-CRT/IMRT(三维适形放射治疗/调强放射治疗)。VMAT技术包括两种剂量输送方法:非连续部分弧形和连续部分弧形。将热释光剂量计(TLD)置于RANDO体模中以估算器官吸收剂量。每种计划技术均应用50.4 Gy的处方剂量并治疗包括肺和心脏在内的关键器官。剂量体积直方图用于显示计划靶体积(V95%)、均匀性指数(HI)、适形指数(CI)及其他优化指标。全身有效剂量的估算基于国际辐射防护委员会(ICRP)第60号和第103号出版物。结果如下:连续部分弧形和非连续部分弧形显示出最佳的CI和HI。连续部分弧形和混合3D-CRT/IMRT中心脏的吸收剂量分别为0.07±0.01%和0%(分别为V5%和V10%)。混合3D-CRT/IMRT中心脏的平均剂量最低(1.47 Gy±0.02)。连续部分弧形中左对侧肺的剂量(V5%)最低(0%)。连续部分弧形中右同侧肺的平均剂量和V20%最低。混合3D-CRT/IMRT对侧乳腺(危及器官)的平均剂量最低。ICRP-60和ICRP-103的全身有效剂量在连续部分弧形中最高(分别为2.01 Sv±0.23和2.89 Sv±0.15)。总之,采用连续弧形的VMAT发生放射性肺炎的风险较低,而混合3D-CRT/IMRT导致继发恶性肿瘤的风险和心血管并发症较低。