Akbaba Sati, Bostel Tilman, Lang Kristin, Bahadir Suzan, Lipman Djoeri, Schmidberger Heinz, Matthias Christoph, Rotter Nicole, Knopf Andreas, Freudlsperger Christian, Plinkert Peter, Debus Juergen, Adeberg Sebastian
Department of Radiation Oncology, University Medical Center Mainz, Mainz, Germany.
Department of Radiation Oncology, University Hospital Heidelberg, Heidelberg, Germany.
Front Oncol. 2020 Nov 11;10:593379. doi: 10.3389/fonc.2020.593379. eCollection 2020.
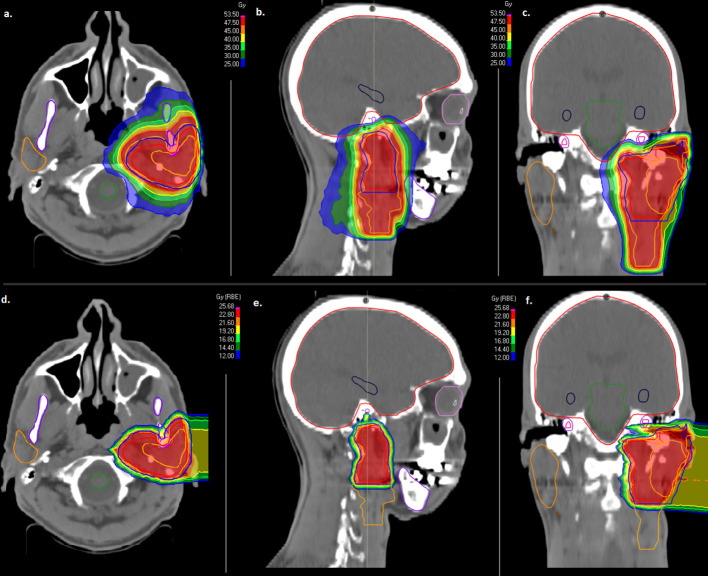
We aimed to evaluate treatment outcome of combined radiotherapy (RT) including photon intensity modulated radiotherapy (IMRT) and carbon ion boost for adenoid cystic carcinomas (ACCs) of the major salivary glands, the currently available largest German collective for this cohort.
Overall, 207 patients who were irradiated with combined RT between 2009 and 2019 at Heidelberg University Hospital were analyzed retrospectively for local control (LC), progression-free survival (PFS) and overall survival (OS) using Kaplan-Meier estimates. The majority of patients received postoperative RT (n=176/207, 85%) after previous surgery in large German hospitals mainly Mainz, Freiburg, Mannheim and Heidelberg University Hospitals and 15% received primary RT (n=31/207).
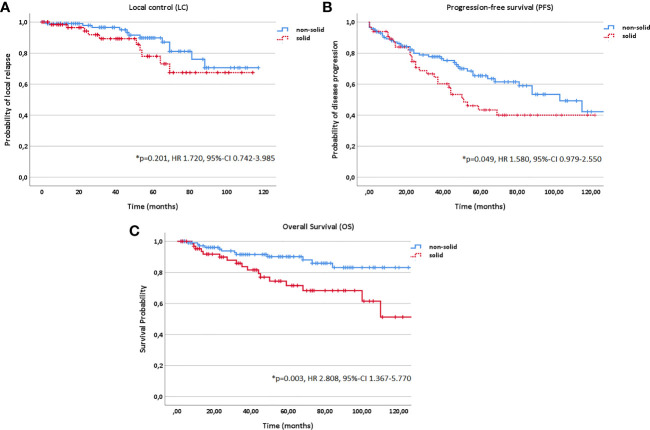
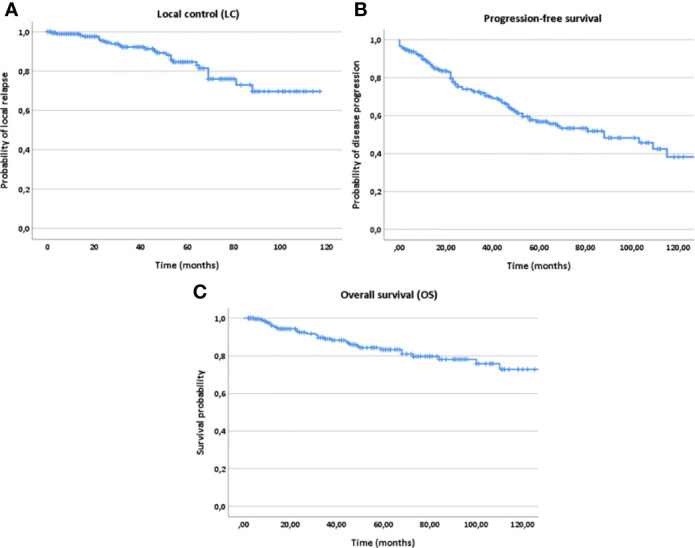
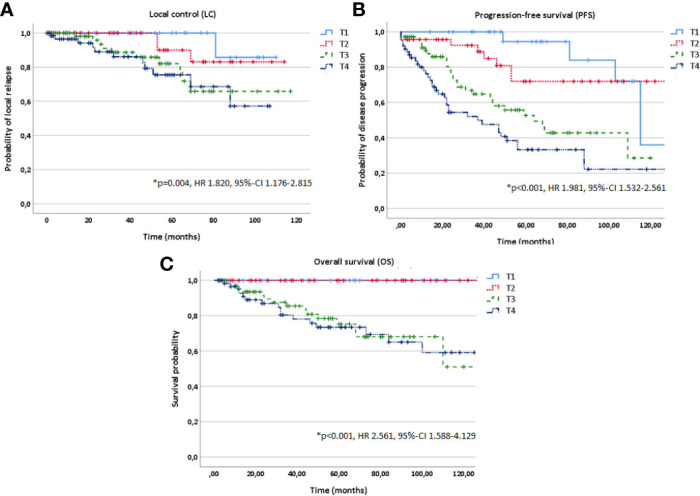
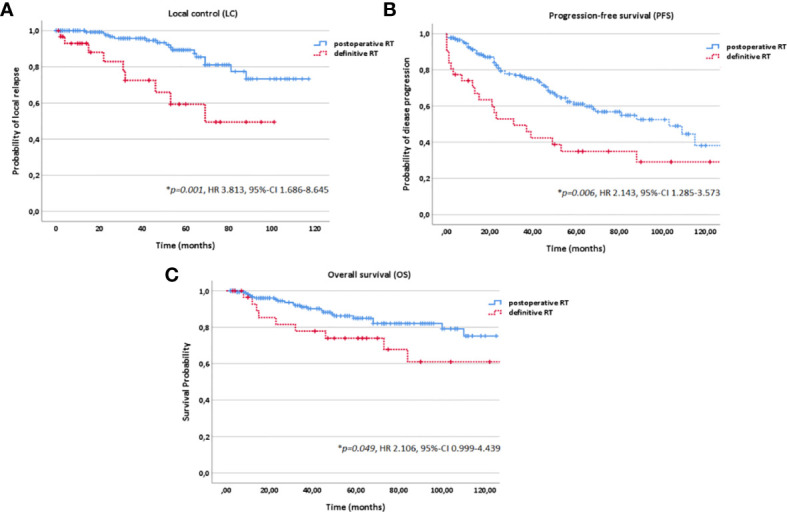
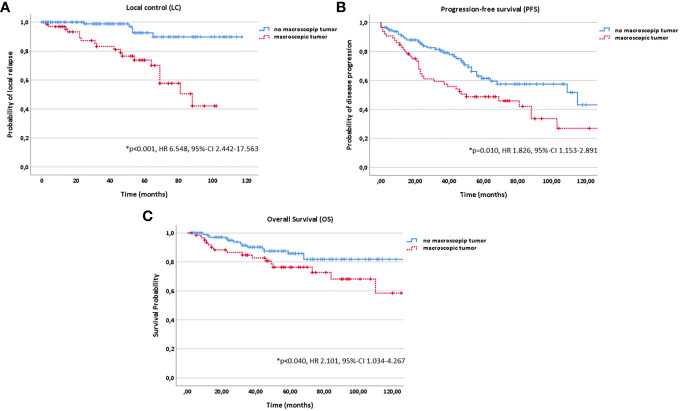
After a median follow-up time of 50 months, 84% of the patients were still alive (n=174/207). Disease progression occurred in 32% of the patients (n=66/207) while local recurrence was diagnosed in 12% (n=25/207), and distant relapse in 27% (n=56/207). Estimated 5-year LC, PFS and OS rates were 84%, 56% and 83% for OS, respectively. In multivariate analysis, we could identify two prognostic subgroups: one subgroup resulting in decreased LC, PFS and OS rates and another subgroup having an additional survival disadvantage in PFS and OS. Patients with a macroscopic tumor disease (yes vs. no; p<0.001 for LC, p=0.010 for PFS and p=0.040 for OS) treated in a definitive setting (vs. postoperative setting; p=0.001 for LC, p=0.006 for PFS, p=0.049 for OS) and tumors of upper T stage (T1-4; p=0.004 for LC, p<0.001 for PFS, p<0.001 for OS) showed significantly more local relapses and a decreased PFS and OS. Upper Age (p<0.001 for both PFS and OS), lower Karnofsky Performance Score (<80% vs. ≥80%; p<0.001 for both PFS and OS) and solid histology (vs. non-solid; p=0.049 for PFS and p=0.003 for OS) were in addition associated with worse survival outcome. Toxicity was moderate with 18% late grade 2 and 3 toxicity.
Combined RT results in superior LC rates compared to photon data with moderate toxicity. In multivariate analysis, upper T stage, the existence of a macroscopic tumor before RT and definitive RT setting were identified as major prognostic factors affecting LC negatively.
我们旨在评估联合放疗(RT)的治疗效果,该联合放疗包括光子调强放疗(IMRT)和碳离子增敏放疗,用于治疗大唾液腺腺样囊性癌(ACC),这是目前德国该队列中可用的最大数据集。
总体而言,对2009年至2019年间在海德堡大学医院接受联合放疗的207例患者进行回顾性分析,使用Kaplan-Meier估计法评估局部控制(LC)、无进展生存期(PFS)和总生存期(OS)。大多数患者(n=176/207,85%)在德国大型医院(主要是美因茨、弗莱堡、曼海姆和海德堡大学医院)先前手术后接受术后放疗,15%的患者接受根治性放疗(n=31/207)。
中位随访时间为50个月后,84%的患者仍存活(n=174/207)。32%的患者发生疾病进展(n=66/207),12%的患者被诊断为局部复发(n=25/207),27%的患者发生远处复发(n=56/207)。估计的5年LC、PFS和OS率分别为84%、56%和83%。在多变量分析中,我们可以识别出两个预后亚组:一个亚组导致LC、PFS和OS率降低,另一个亚组在PFS和OS方面有额外的生存劣势。在根治性治疗(与术后治疗相比;LC的p=0.001,PFS的p=0.006,OS的p=0.049)中治疗的有肉眼可见肿瘤疾病的患者(是与否;LC的p<0.001,PFS的p=0.010,OS的p=0.040)以及T分期较高的肿瘤(T1-4;LC的p=0.004,PFS的p<0.001,OS的p<0.001)显示出明显更多的局部复发以及PFS和OS降低。高龄(PFS和OS均p<0.001)、较低的卡氏功能状态评分(<80%与≥80%;PFS和OS均p<0.001)和实体组织学(与非实体相比;PFS的p=0.049,OS的p=0.003)此外还与较差的生存结果相关。毒性为中度,18%为晚期2级和3级毒性。
与光子放疗数据相比,联合放疗导致更高的LC率且毒性中度。在多变量分析中,较高的T分期、放疗前存在肉眼可见肿瘤以及根治性放疗设置被确定为对LC有负面影响的主要预后因素。