The Primary Care Unit, Department of Public Health and Primary Care, University of Cambridge, Cambridge, UK.
University of Cambridge School of Clinical Medicine, Addenbrooke's Hospital, Cambridge, UK.
Health Expect. 2021 Apr;24(2):341-351. doi: 10.1111/hex.13175. Epub 2020 Dec 2.
Using risk stratification approaches to determine eligibility has the potential to improve efficiency of screening.
To compare the public acceptability and potential impact on uptake of using different approaches to determine eligibility for screening.
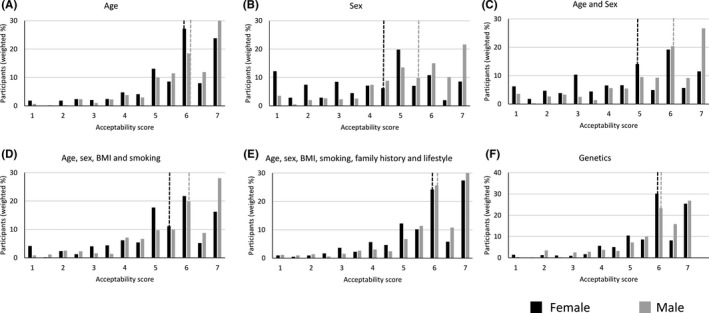
An online population-based survey of 668 adults in the UK aged 45-79 including a series of scenarios in the context of a potential kidney cancer screening programme in which eligibility was determined by age, sex, age and sex combined, a simple risk score (age, sex, body mass index, smoking status), a complex risk score additionally incorporating family history and lifestyle, or a genetic risk score.
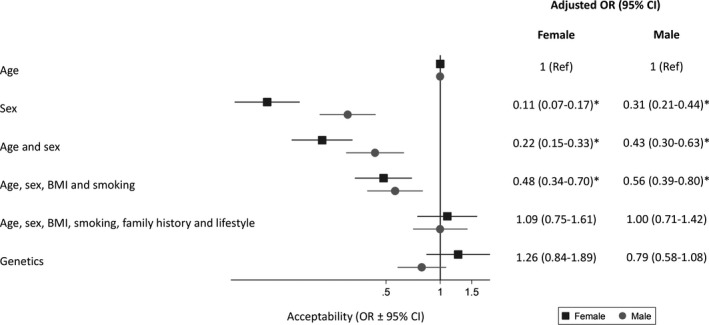
We used multi-level ordinal logistic regression to compare acceptability and potential uptake within individuals and multivariable ordinal logistic regression differences between individuals.
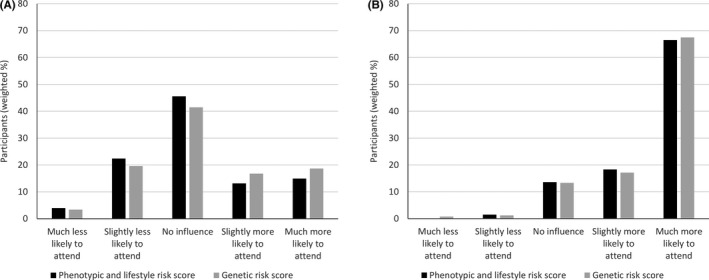
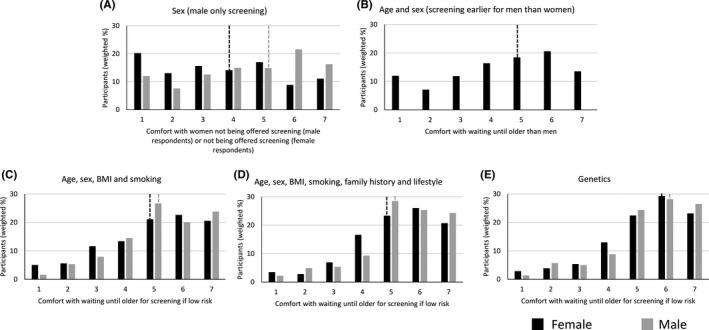
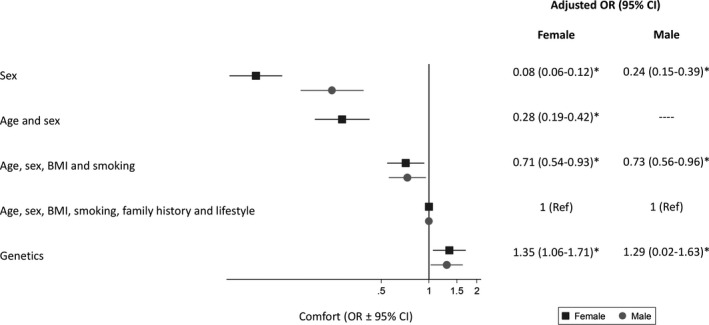
Using sex, age and sex, or the simple risk score were less acceptable than age (P < .0001). All approaches were less acceptable to women than men. Over 70% were comfortable waiting until they were older if the complex risk score or genetics indicated a low risk. If told they were high risk, 85% would be more likely to take up screening. Being told they were low risk had no overall influence on uptake.
Varying the starting age of screening based on estimated risk from models incorporating phenotypic or genetic risk factors would be acceptable to most individuals and may increase uptake.
Two members of the public contributed to the development of the survey and have commented on this paper.
使用风险分层方法来确定资格具有提高筛选效率的潜力。
比较使用不同方法确定筛选资格的公众接受程度和对参与度的潜在影响。
在英国,对 668 名 45-79 岁的成年人进行了一项基于人群的在线调查,其中包括一系列潜在肾癌筛查计划中的情景,这些情景中通过年龄、性别、年龄和性别结合、简单风险评分(年龄、性别、体重指数、吸烟状况)、复杂风险评分(另外纳入家族史和生活方式)或遗传风险评分来确定资格。
我们使用多水平有序逻辑回归来比较个体内的可接受性和潜在参与度,并使用多变量有序逻辑回归来比较个体间的差异。
与年龄相比,使用性别、年龄和性别或简单风险评分的可接受性较低(P<.0001)。所有方法对女性的可接受性都低于男性。如果复杂风险评分或遗传因素表明风险较低,超过 70%的人愿意等待更年长时再进行筛查。如果被告知自己的风险较高,85%的人更有可能接受筛查。被告知自己的风险较低不会对参与度产生总体影响。
根据纳入表型或遗传风险因素的模型估计的风险,改变筛查的起始年龄可能会被大多数人接受,并可能增加参与度。
两名公众参与了调查的开发,并对本文发表了评论。