Department of Medicine, Weill Cornell Medicine, New York (M.M.S., E.R., M.R.S., L.C.P.).
Department of Surgery (J.S.R.), University of Alabama at Birmingham Medical School.
Circulation. 2021 Jan 19;143(3):244-253. doi: 10.1161/CIRCULATIONAHA.120.048026. Epub 2020 Dec 3.
Social determinants of health (SDH) are individually associated with incident coronary heart disease (CHD) events. Indices reflecting social deprivation have been developed for population management, but are difficult to operationalize during clinical care. We examined whether a simple count of SDH is associated with fatal incident CHD and nonfatal myocardial infarction (MI).
We used data from the prospective longitudinal REGARDS cohort study (Reasons for Geographic and Racial Differences in Stroke), a national population-based sample of community-dwelling Black and White adults age ≥45 years recruited from 2003 to 2007. Seven SDH from the 5 Healthy People 2020 domains included social context (Black race, social isolation); education (educational attainment); economic stability (annual household income); neighborhood (living in a zip code with high poverty); and health care (lacking health insurance, living in 1 of the 9 US states with the least public health infrastructure). Outcomes were expert adjudicated fatal incident CHD and nonfatal MI.
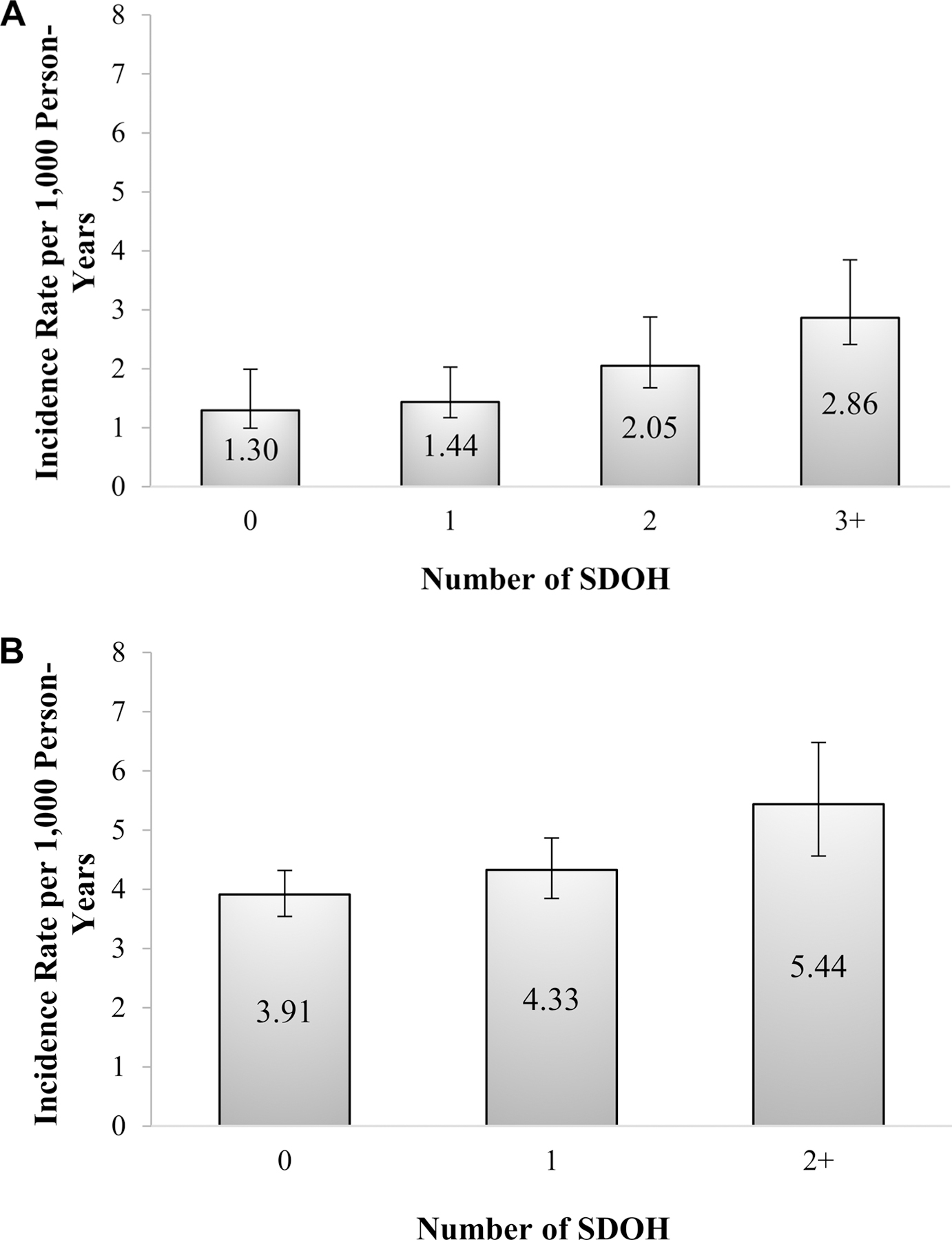
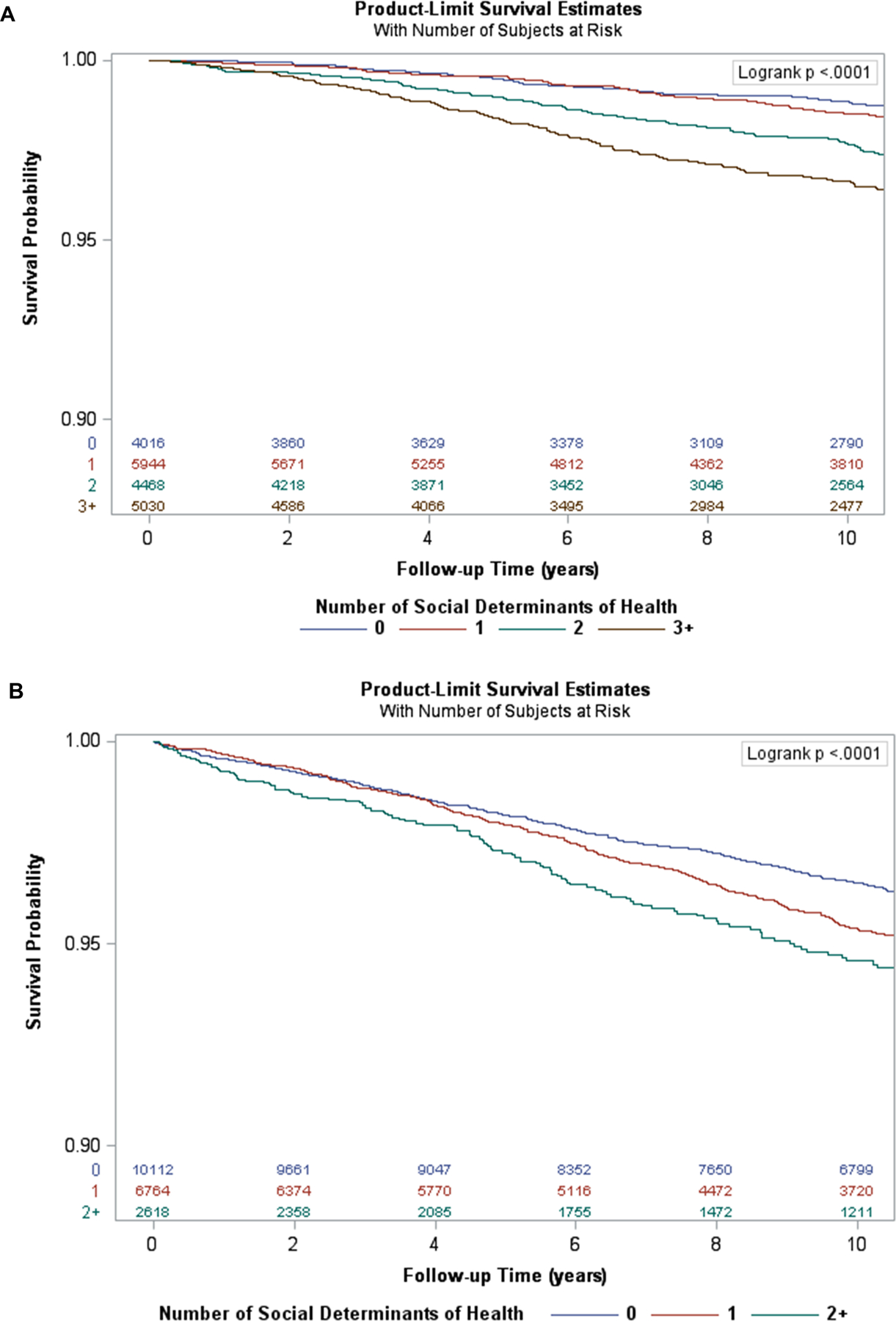
Of 22 152 participants free of CHD at baseline, 58.8% were women and 42.0% were Black; 20.6% had no SDH, 30.6% had 1, 23.0% had 2, and 25.8% had ≥3. There were 463 fatal incident CHD events and 932 nonfatal MIs over a median of 10.7 years (interquartile range, 6.6 to 12.7). Fewer SDHs were associated with nonfatal MI than with fatal incident CHD. The age-adjusted incidence per 1000 person-years increased with the number of SDH for both fatal incident CHD (0 SDH, 1.30; 1 SDH, 1.44; 2 SDH, 2.05; ≥3 SDH, 2.86) and nonfatal MI (0 SDH, 3.91; 1 SDH, 4.33; ≥2 SDH, 5.44). Compared with those without SDH, crude and fully adjusted hazard ratios for fatal incident CHD among those with ≥3 SDH were 3.00 (95% CI, 2.17 to 4.15) and 1.67 (95% CI, 1.18 to 2.37), respectively; hazard ratios for nonfatal MI among those with ≥2 SDH were 1.57 (95% CI, 1.30 to 1.90) and 1.14 (95% CI, 0.93 to 1.41), respectively.
A greater burden of SDH was associated with a graded increase in risk of incident CHD, with greater magnitude and independent associations for fatal incident CHD. Counting the number of SDHs may be a promising approach that could be incorporated into clinical care to identify individuals at high risk of CHD.
健康的社会决定因素(SDH)与冠心病(CHD)事件的发生有个体相关性。反映社会剥夺的指数已经开发出来用于人群管理,但在临床护理中很难实施。我们研究了简单计数 SDH 是否与致命性冠心病和非致命性心肌梗死(MI)有关。
我们使用了来自前瞻性纵向 REGARDS 队列研究(地理和种族差异中风的原因)的数据,这是一项全国性的基于社区的黑人和白人成年人样本,年龄≥45 岁,于 2003 年至 2007 年招募。五个健康人 2020 年目标领域中的七个 SDH 包括社会背景(黑人种族,社会孤立);教育(教育程度);经济稳定(家庭年收入);邻里(居住在贫困率高的邮政编码中);以及医疗保健(没有医疗保险,居住在美国九个公共卫生基础设施最少的州之一)。结果是专家裁定的致命性冠心病和非致命性 MI。
在基线时没有冠心病的 22152 名参与者中,58.8%是女性,42.0%是黑人;20.6%没有 SDH,30.6%有 1 个,23.0%有 2 个,25.8%有≥3 个。中位数为 10.7 年(四分位距,6.6 至 12.7)期间,共发生 463 例致命性冠心病事件和 932 例非致命性心肌梗死。与致命性冠心病相比,SDH 较少与非致命性 MI 相关。在年龄调整后,每 1000 人年的发病率随 SDH 数量的增加而增加,包括致命性冠心病(0 SDH,1.30;1 SDH,1.44;2 SDH,2.05;≥3 SDH,2.86)和非致命性 MI(0 SDH,3.91;1 SDH,4.33;≥2 SDH,5.44)。与没有 SDH 的人相比,在≥3 SDH 的人中,致命性冠心病的粗和完全调整后的危险比分别为 3.00(95%CI,2.17 至 4.15)和 1.67(95%CI,1.18 至 2.37);在≥2 SDH 的人中,非致命性 MI 的危险比分别为 1.57(95%CI,1.30 至 1.90)和 1.14(95%CI,0.93 至 1.41)。
SDH 负担增加与冠心病事件风险呈梯度增加相关,致命性冠心病的相关性更强,独立相关性更大。计数 SDH 的数量可能是一种很有前途的方法,可以纳入临床护理,以识别冠心病风险高的个体。