Razavi Moaven, O'Reilly-Jacob Monica, Perloff Jennifer, Buerhaus Peter
The Heller School for Social Policy and Management, Brandeis University, Waltham.
William F. Connell School of Nursing, Boston College, Chestnut Hill, MA.
Med Care. 2021 Feb 1;59(2):177-184. doi: 10.1097/MLR.0000000000001477.
Although recent research suggests that primary care provided by nurse practitioners costs less than primary care provided by physicians, little is known about underlying drivers of these cost differences.
Identify the drivers of cost differences between Medicare beneficiaries attributed to primary care nurse practitioners (PCNPs) and primary care physicians (PCMDs).
Cross-sectional cost decomposition analysis using 2009-2010 Medicare administrative claims for beneficiaries attributed to PCNPs and PCMDs with risk stratification to control for beneficiary severity. Cost differences between PCNPs and PCMDs were decomposed into payment, service volume, and service mix within low-risk, moderate-risk and high-risk strata.
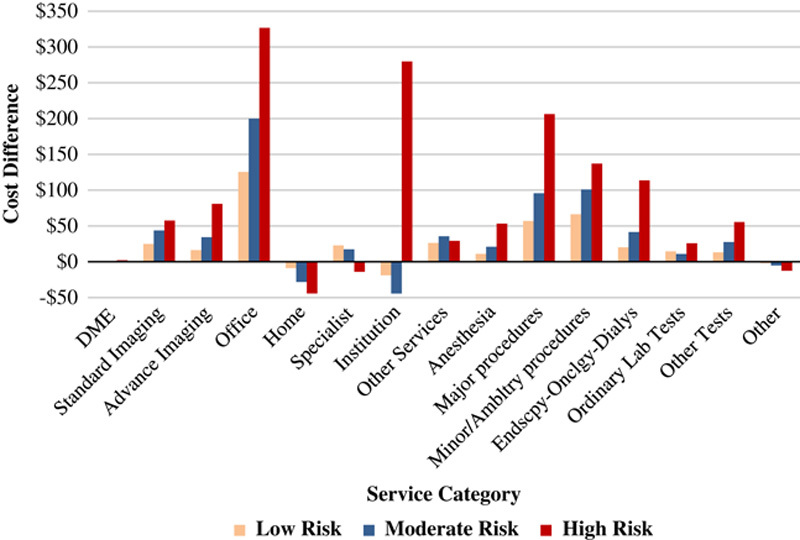
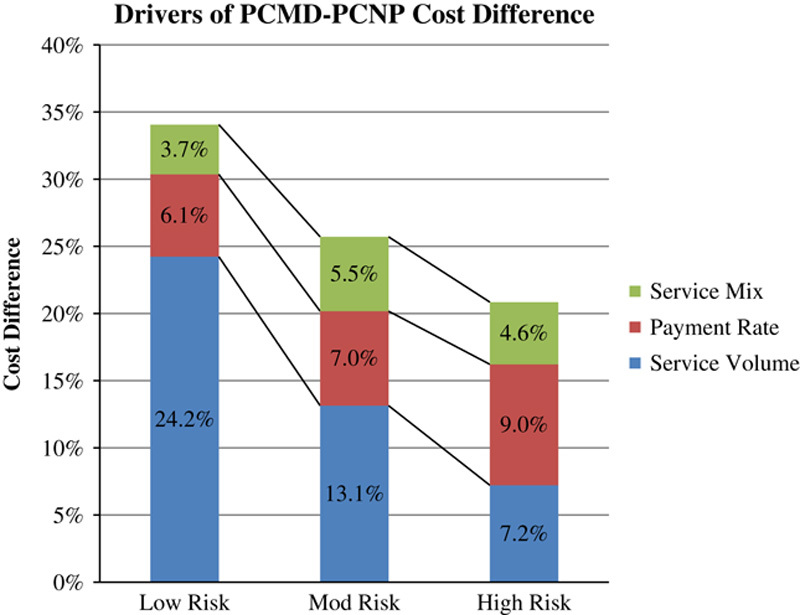
Overall, the average PCMD cost of care is 34% higher than PCNP care in the low-risk stratum, and 28% and 21% higher in the medium-risk and high-risk stratum. In the low-risk stratum, the difference is comprised of 24% service volume, 6% payment, and 4% service mix. In the high-risk stratum, the difference is composed of 7% service volume, 9% payment, and 4% service mix. The cost difference between PCNP and PCMD attributed beneficiaries is persistent and significant, but narrows as risk increases. Across the strata, PCNPs use fewer and less expensive services than PCMDs. In the low-risk stratum, PCNPs use markedly fewer services than PCMDs.
There are differences in the costs of primary care of Medicare beneficiaries provided by nurse practitioners and MDs. Especially in low-risk populations, the lower cost of PCNP provided care is primarily driven by lower service volume.
尽管近期研究表明,执业护士提供的初级护理成本低于医生提供的初级护理成本,但对于这些成本差异的潜在驱动因素知之甚少。
确定医疗保险受益人中,初级护理执业护士(PCNP)和初级护理医生(PCMD)之间成本差异的驱动因素。
采用2009 - 2010年医疗保险行政索赔数据,对归因于PCNP和PCMD的受益人进行横断面成本分解分析,并进行风险分层以控制受益人的病情严重程度。PCNP和PCMD之间的成本差异被分解为低风险、中等风险和高风险分层内的支付、服务量和服务组合。
总体而言,在低风险分层中,PCMD的平均护理成本比PCNP护理高34%,在中等风险和高风险分层中分别高28%和21%。在低风险分层中,差异由24%的服务量、6%的支付和4%的服务组合构成。在高风险分层中,差异由7%的服务量、9%的支付和4%的服务组合构成。PCNP和PCMD归因受益人的成本差异持续且显著,但随着风险增加而缩小。在各分层中,PCNP使用的服务比PCMD少且成本低。在低风险分层中,PCNP使用的服务明显少于PCMD。
执业护士和医生为医疗保险受益人提供的初级护理成本存在差异。特别是在低风险人群中,PCNP提供护理的低成本主要是由较低的服务量驱动的。