Department of Orthopaedic Surgery, New Taipei Municipal TuCheng Hospital, New Taipei, 236, Taiwan, ROC.
Bone and Joint Research Center, Linkou Chang Gung Memorial Hospital and Chang Gung University College of Medicine, Taoyuan, 333, Taiwan, ROC.
Sci Rep. 2020 Dec 3;10(1):21188. doi: 10.1038/s41598-020-78139-y.
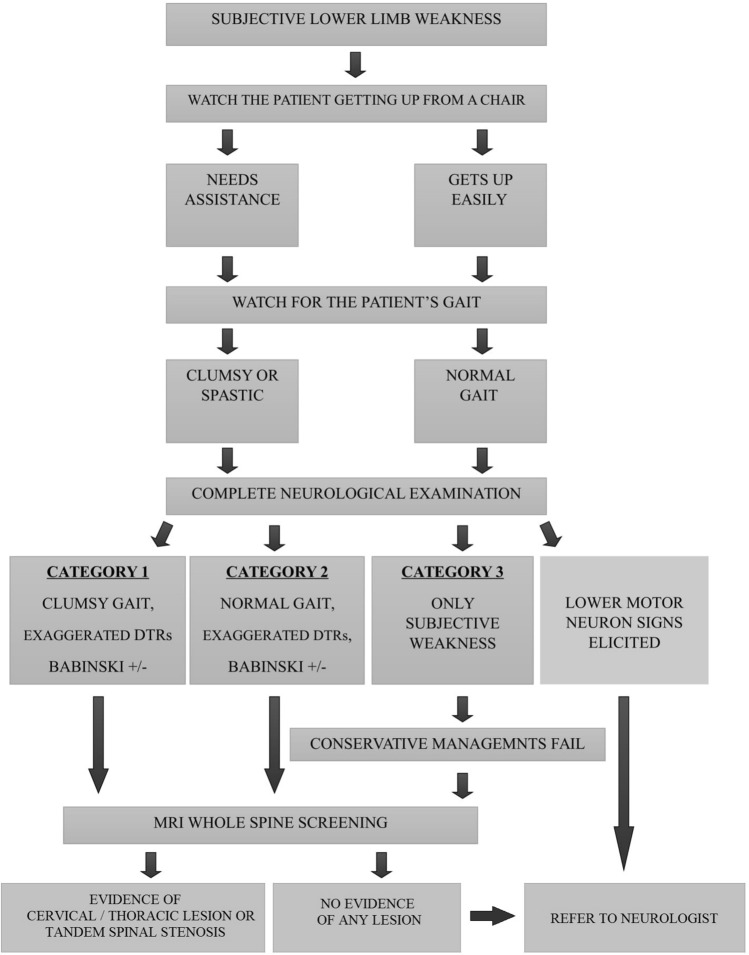
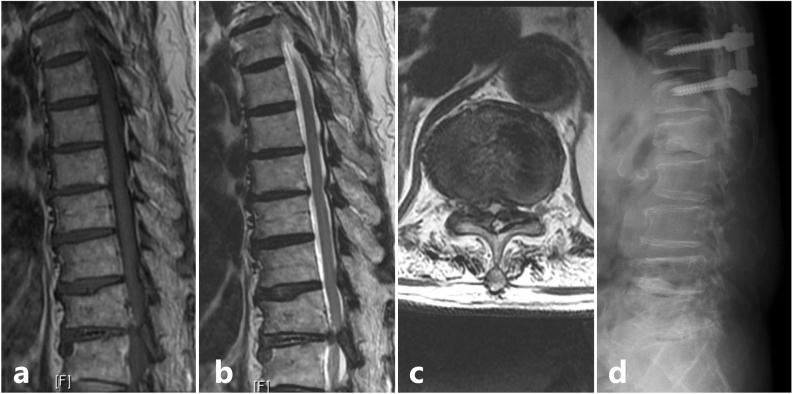
When patients presenting with subjective lower limb weakness (SLLW) are encountered, it is natural to suspect a lumbar pathology and proceed with related clinical examination, investigations and management. However, SLLW could be a sign of degenerative cervical myelopathy (DCM) due to an evolving cord compression. In such circumstances, if symptoms are not correlated to myelopathy at the earliest, there could be potential complications over time. In this study, we intend to analyse the outcomes after surgical management of the cervical or thoracic cord compression in patients with SLLW. Retrospectively, patients who presented to our center during the years 2010-2016 with sole complaint of bilateral SLLW but radiologically diagnosed to have a solitary cervical or thoracic stenosis, or tandem spinal stenosis and underwent surgical decompression procedures were selected. Their clinical presentation was categorised into three types, myelopathy was graded using Nurick's grading and JOA scoring; in addition, their lower limb functional status was assessed using the lower extremity functional scale (LEFS). Functional recovery following surgery was assessed at 6 weeks, 3 months, 6 months, one year, and two years. Selected patients (n = 24; Age, 56.4 ± 10.1 years; range 32-78 years) had SLLW for a period of 6.4 ± 3.2 months (range 2-13 months). Their preoperative JOA score was 11.3 ± 1.8 (range 7-15), and LEFS was 34.4 ± 7.7 (range 20-46). Radiological evidence of a solitary cervical lesion and tandem spinal stenosis was found in 6 and 18 patients respectively. Patients gradually recovered after surgical decompression with LEFS 59.8 ± 2.7 (range 56-65) at 1 year and JOA score 13.6 ± 2.7 (range - 17 to 100) at 2 years. The recovery rate at final follow up was 47.5%. Our results indicate the importance of clinically suspecting SLLW as an early non-specific sign of DCM to avoid misdiagnosis, especially in patients without conventional upper motor neuron signs. In such cases, surgical management of the cord compression resulted in significant functional recovery and halted the progression towards permanent disability.
当遇到出现主观下肢无力(SLLW)的患者时,自然会怀疑是腰椎病变,并进行相关的临床检查、检查和管理。然而,SLLW 也可能是由于脊髓受压而导致的退行性颈椎脊髓病(DCM)的迹象。在这种情况下,如果症状在早期与脊髓病不相关,随着时间的推移可能会出现潜在的并发症。在这项研究中,我们旨在分析 SLLW 患者颈椎或胸椎脊髓压迫症手术治疗后的结果。回顾性地选择了 2010 年至 2016 年期间因单纯双侧 SLLW 就诊但影像学诊断为单一颈椎或胸椎狭窄、或串联脊髓狭窄并接受手术减压治疗的患者。他们的临床表现分为三种类型,使用 Nurick 分级和 JOA 评分对脊髓病进行分级;此外,使用下肢功能量表(LEFS)评估他们的下肢功能状况。术后 6 周、3 个月、6 个月、1 年和 2 年评估手术的功能恢复情况。选择的患者(n=24;年龄 56.4±10.1 岁;范围 32-78 岁)有 SLLW 病史 6.4±3.2 个月(范围 2-13 个月)。他们的术前 JOA 评分为 11.3±1.8(范围 7-15),LEFS 评分为 34.4±7.7(范围 20-46)。6 例和 18 例患者分别发现有单一颈椎病变和串联脊髓狭窄的放射学证据。患者在手术后逐渐恢复,1 年后的 LEFS 为 59.8±2.7(范围 56-65),2 年后的 JOA 评分为 13.6±2.7(范围-17 至 100)。最终随访时的恢复率为 47.5%。我们的结果表明,临床上怀疑 SLLW 是 DCM 的早期非特异性征象的重要性,以避免误诊,特别是在没有传统上运动神经元体征的患者中。在这种情况下,脊髓压迫的手术治疗可显著恢复功能,并阻止向永久性残疾发展。