Fligor Scott C, Tsikis Savas T, Wang Sophie, Ore Ana Sofia, Allar Benjamin G, Whitlock Ashlyn E, Calvillo-Ortiz Rodrigo, Arndt Kevin, Callery Mark P, Gangadharan Sidhu P
Department of Surgery, Beth Israel Deaconess Medical Center, Harvard Medical School, Boston, MA, USA.
J Thorac Dis. 2020 Nov;12(11):6640-6654. doi: 10.21037/jtd-20-2400.
Coronavirus disease 2019 (COVID-19) has overwhelmed hospital resources worldwide, requiring widespread cancellation of non-emergency operations, including lung and esophageal cancer operations. In the United States, while hospitals begin to increase surgical volume and tackle the backlog of cases, the specter of a "second wave," with a potential vaccine months to years away, highlights the ongoing need to triage cases based upon the risk of surgical delay. We synthesize the available literature on time to surgery and its impact on outcomes along with a critical appraisal of the released triage guidelines in the United States.
We performed a systematic literature review using PubMed according to preferred reporting items for systematic reviews and meta-analyses guidelines evaluating relevant literature from the past 15 years.
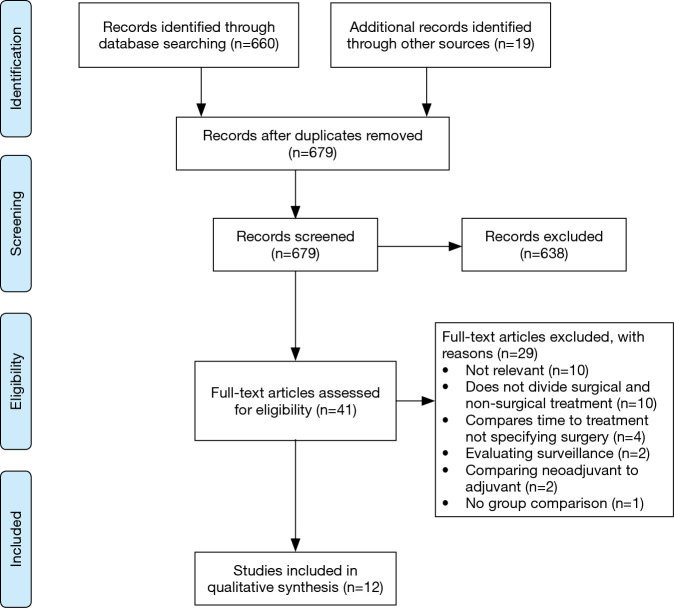
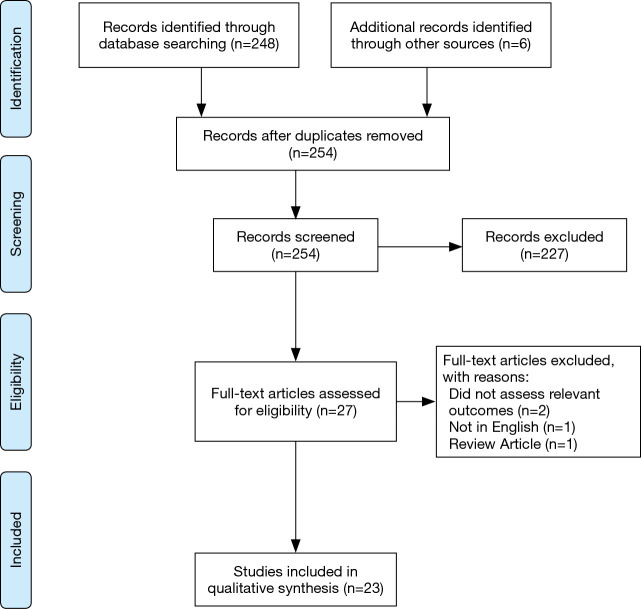
Out of 679 screened abstracts, 12 studies investigating time to surgery in lung cancer were included. In stage I-II lung cancer, delayed resection beyond 6 to 8 weeks is consistently associated with lower survival. No identified evidence justifies a 2 cm cutoff for immediate versus delayed surgery. For stage IIIa lung cancer, time to surgery greater than 6 weeks after neoadjuvant therapy is similarly associated with worse survival. For esophageal cancer, 254 abstracts were screened and 23 studies were included. Minimal literature addresses primary esophagectomy, but time to surgery over 8 weeks is associated with lower survival. In the neoadjuvant setting, longer time to surgery is associated with increased pathologic complete response, but also decreased survival. The optimal window for esophagectomy following neoadjuvant therapy is 6 to 8 weeks.
In the setting of the COVID-19 pandemic, timely resection of lung and esophageal cancer should be prioritized whenever possible based upon local resources and disease-burden.
2019年冠状病毒病(COVID-19)使全球医院资源不堪重负,导致包括肺癌和食管癌手术在内的非紧急手术普遍取消。在美国,尽管医院开始增加手术量并处理积压病例,但在距离潜在疫苗问世还有数月至数年的情况下,“第二波疫情”的幽灵凸显了根据手术延迟风险对病例进行分类的持续必要性。我们综合了关于手术时机及其对预后影响的现有文献,并对美国发布的分类指南进行了批判性评估。
我们根据系统评价和荟萃分析的首选报告项目,使用PubMed对过去15年的相关文献进行了系统的文献综述。
在679篇筛选出的摘要中,纳入了12项关于肺癌手术时机的研究。在I-II期肺癌中,手术延迟超过6至8周与生存率降低始终相关。没有明确证据证明立即手术与延迟手术的2厘米界限合理。对于IIIa期肺癌,新辅助治疗后手术时间超过6周同样与较差的生存率相关。对于食管癌,筛选了254篇摘要,纳入了23项研究。关于原发性食管癌切除术的文献极少,但手术时间超过8周与生存率降低相关。在新辅助治疗情况下,手术时间延长与病理完全缓解率增加相关,但也与生存率降低相关。新辅助治疗后食管癌切除术的最佳时间窗是6至8周。
在COVID-19大流行的背景下,应根据当地资源和疾病负担,尽可能优先及时切除肺癌和食管癌。