Hassanzadeh Comron, Sita Timothy, Savoor Rohan, Samson Pamela P, Bradley Jeffrey, Gentile Michelle, Roach Michael, Mohindra Nisha, Waqar Saiama, Kruser Timothy J, Robinson Clifford
Department of Radiation Oncology, Washington University School of Medicine, St. Louis, MO, USA.
Department of Radiation Oncology, Northwestern Memorial Hospital, Chicago, IL, USA.
J Thorac Dis. 2020 Nov;12(11):6690-6700. doi: 10.21037/jtd-20-1792.
Consolidation durvalumab improved overall survival (OS) in locally advanced non-small cell lung cancer (LA-NSCLC) treated with chemoradiotherapy (CRT) in the PACIFIC trial; however, pneumonitis was increased with durvalumab. We sought to examine real-world outcomes with the PACIFIC paradigm, especially factors associated with pneumonitis, using a multi-institutional review.
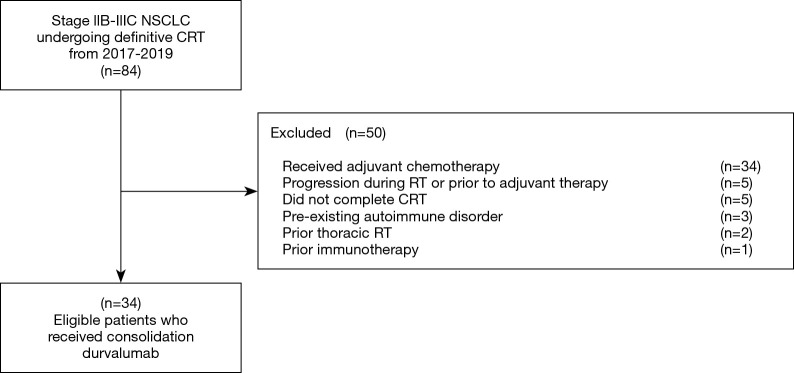
Patients with LA-NSCLC treated with CRT followed by durvalumab from January 2017-February 2019 were identified at 2 institutions. We characterized demographics, tumor factors, radiotherapy, and duration of durvalumab. We examined pneumonitis outcomes including re-challenge success, with secondary endpoints of progression-free survival (PFS) and OS.
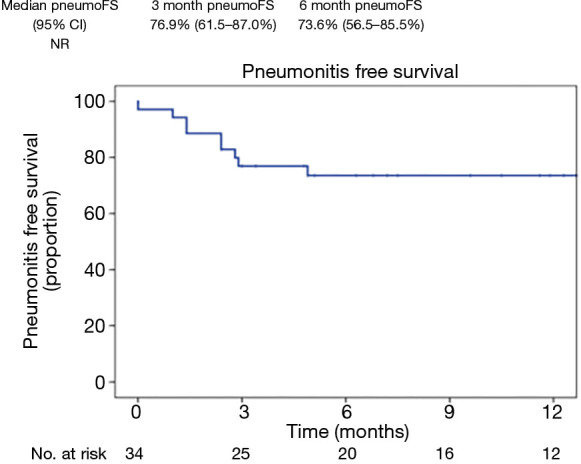
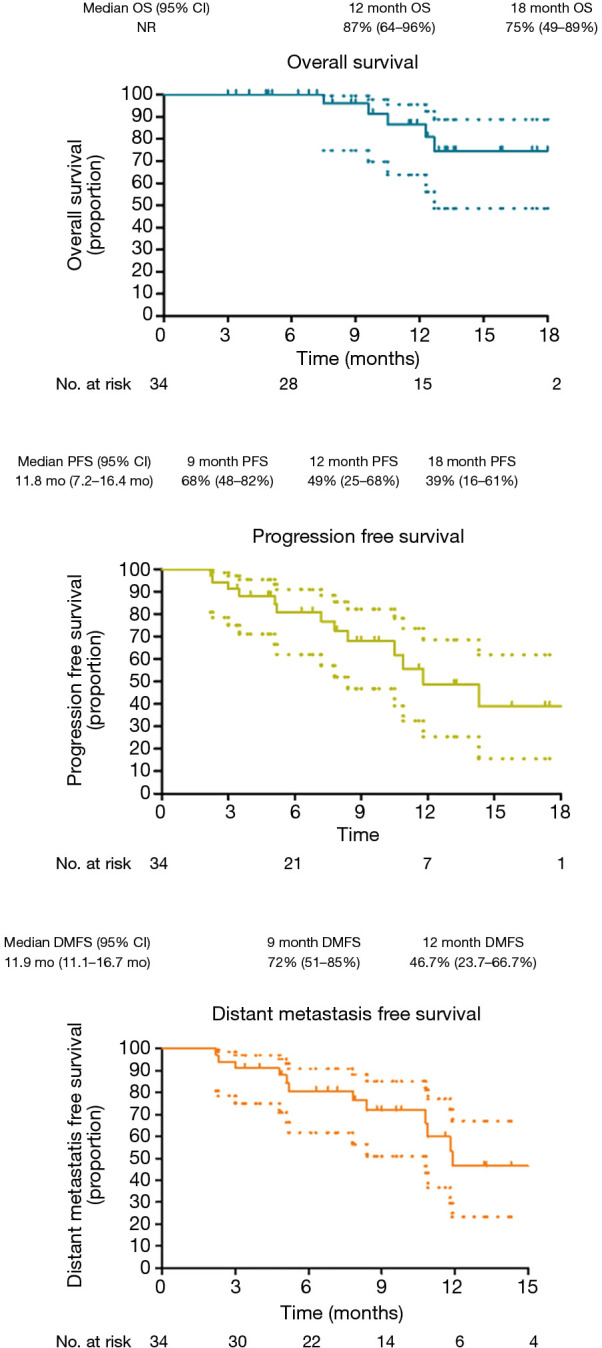
Thirty-four patients were included with median follow-up of 12 months (range, 3 to 20 months); 94% had stage III disease. The cumulative grade >2 pneumonitis rate was 26.5% with 2 patients developing grade 3 pneumonitis and no grade 4/5 events. Median time to pneumonitis after RT was 2.4 months (range, 0 to 4.9 months). Pneumonitis management included median prednisone dose of 60 mg for median taper of 6 weeks with durvalumab held for median of 4.5 weeks (range, 2 to 8 weeks); 70% of pneumonitis patients received durvalumab re-challenge, with pneumonitis recurring in 14% of patients. 3-month and 6-month pneumonitis-free-survival were 76.9% and 73.6%, respectively; 9- and 12-month OS were 96% (75.1-99.8%), 86.6% (63.5-95.5%), respectively; 9- and 12-month PFS were 68% (47.5-82.5%), 48.7% (25.3-68.3%). Pneumonitis development did not significantly impact PFS or OS (P>0.05).
Among LA-NSCLC patients treated with CRT followed by consolidation durvalumab, more than 25% developed symptomatic pneumonitis. In this small case series, pneumonitis did not appear to negatively impact survival, and durvalumab re-challenge appeared feasible after pneumonitis treatment with steroids.
在 PACIFIC 试验中,度伐利尤单抗巩固治疗可改善接受放化疗(CRT)的局部晚期非小细胞肺癌(LA-NSCLC)患者的总生存期(OS);然而,度伐利尤单抗会增加肺炎的发生风险。我们试图通过多机构回顾来研究采用 PACIFIC 模式的真实世界结局,尤其是与肺炎相关的因素。
在两家机构中确定了 2017 年 1 月至 2019 年 2 月期间接受 CRT 后使用度伐利尤单抗治疗的 LA-NSCLC 患者。我们对患者的人口统计学特征、肿瘤因素、放疗情况以及度伐利尤单抗的使用时长进行了描述。我们研究了肺炎结局,包括再次使用成功情况,并将无进展生存期(PFS)和 OS 作为次要终点。
共纳入 34 例患者,中位随访时间为 12 个月(范围 3 至 20 个月);94%为 III 期疾病。累积 2 级以上肺炎发生率为 26.5%,2 例患者发生 3 级肺炎,无 4/5 级事件。放疗后发生肺炎的中位时间为 2.4 个月(范围 0 至 4.9 个月)。肺炎的治疗包括泼尼松中位剂量为 60mg,中位减量期为 6 周,度伐利尤单抗中位停药时间为 4.5 周(范围 2 至 8 周);70%的肺炎患者接受了度伐利尤单抗再次使用,其中 14%的患者肺炎复发。3 个月和 6 个月无肺炎生存率分别为 76.9%和 73.6%;9 个月和 12 个月 OS 分别为 96%(75.1 - 99.8%)、86.6%(63.5 - 95.5%);9 个月和 12 个月 PFS 分别为 68%(47.5 - 82.5%)、48.7%(25.3 - 68.3%)。肺炎的发生对 PFS 或 OS 无显著影响(P>0.05)。
在接受 CRT 后使用度伐利尤单抗巩固治疗的 LA-NSCLC 患者中,超过 25%发生了有症状的肺炎。在这个小病例系列中,肺炎似乎并未对生存产生负面影响,并且在使用类固醇治疗肺炎后,度伐利尤单抗再次使用似乎是可行的。