Owen Dawn, Sio Terence T
Department of Radiation Oncology, Mayo Clinic, Rochester, Minnesota, USA.
Department of Radiation Oncology, Mayo Clinic, Phoenix, Arizona, USA.
J Thorac Dis. 2020 Nov;12(11):7024-7031. doi: 10.21037/jtd-2019-cptn-01.
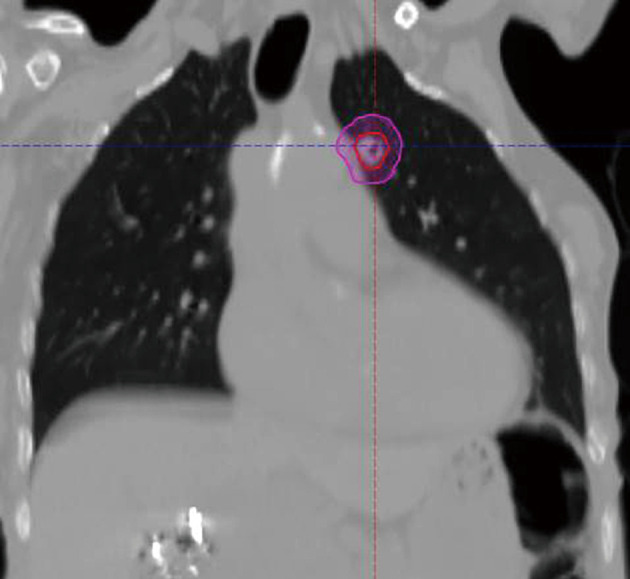
Advancements in imaging and radiotherapy (RT) techniques have allowed for remarkably precise delivery of high radiation dose per treatment fraction to intrathoracic targets. As a non-invasive therapeutic modality (compared to surgery), stereotactic body radiotherapy (SBRT) is an attractive option for patients with early-stage non-small cell lung cancers and oligometastases, especially for older patients with significant comorbidities and pre-existing pulmonary dysfunction. However, the outcomes and side effect profile of SBRT are highly dependent on tumor location, especially if the tumor is located centrally (within 2 cm of the proximal bronchial tree (PBT)] or ultracentrally (touching or within 1 cm of the mediastinum, esophagus, and PBT). In this focused review, we will examine the contemporary practice and principles of using hypofractionated RT or SBRT for central and ultracentral thoracic tumors. We will identify future directions on how this practice may be incorporated into the increasingly complicated modern paradigm of lung cancer treatments which now include immunotherapy along with proton beam radiotherapy.
成像和放射治疗(RT)技术的进步使得每次治疗分割能够非常精确地向胸内靶区输送高辐射剂量。作为一种非侵入性治疗方式(与手术相比),立体定向体部放射治疗(SBRT)对于早期非小细胞肺癌和寡转移患者是一个有吸引力的选择,特别是对于有严重合并症和既往存在肺功能障碍的老年患者。然而,SBRT的疗效和副作用情况高度依赖于肿瘤位置,特别是如果肿瘤位于中央(距近端支气管树(PBT)2 cm以内)或超中央(接触纵隔、食管和PBT或在其1 cm范围内)。在这篇重点综述中,我们将探讨对中央和超中央胸部肿瘤使用低分割放疗或SBRT的当代实践和原则。我们将确定关于如何将这种实践纳入日益复杂的现代肺癌治疗模式的未来方向,现在肺癌治疗模式包括免疫治疗以及质子束放疗。