Ono Kosei, Shimizu Takayoshi, Fujibayashi Shunsuke, Otsuki Bungo, Murata Koichi, Sakamoto Akio, Matsuda Shuichi
Department of Orthopaedic Surgery, Kyoto University, Graduate School of Medicine, Kyoto, Japan.
Neurospine. 2021 Mar;18(1):163-169. doi: 10.14245/ns.2040494.247. Epub 2020 Dec 4.
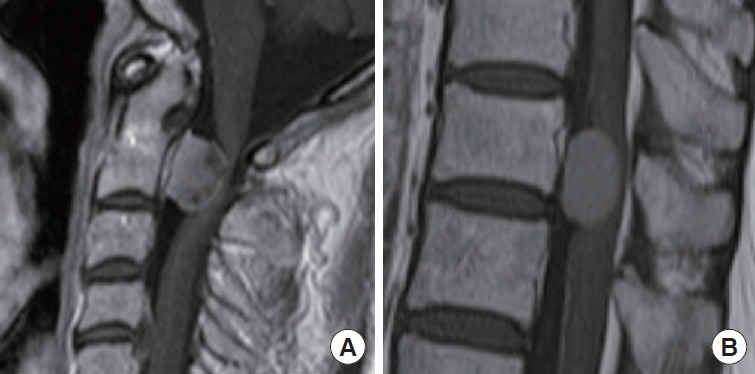
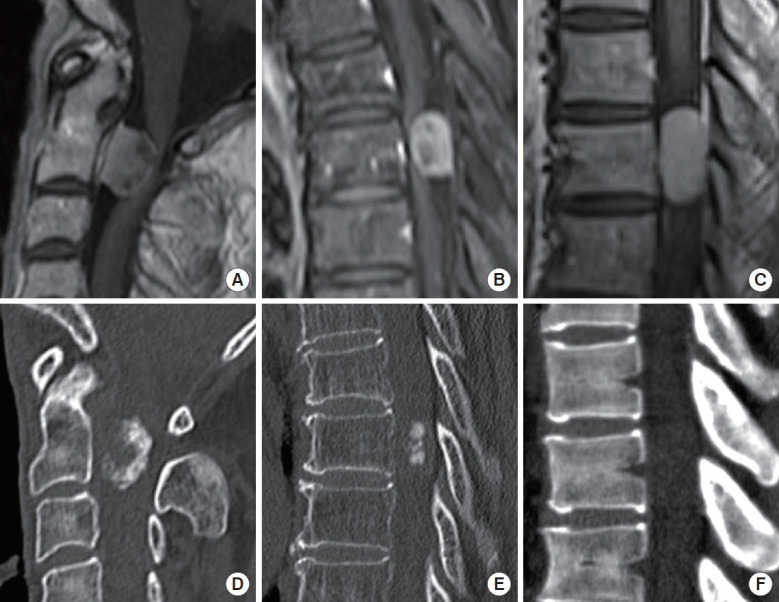
Spinal meningioma is mostly benign, but they can exhibit neurological deficit. The relationship between neurological impairment and its radiographic findings, including intratumor magnetic resonance imaging (MRI) gadolinium enhancement and calcification in computed tomography (CT) scan, has not been studied. The purpose of this study was to investigate the association of preoperative image findings with neurological status in spinal meningioma.
Patients histologically diagnosed with spinal meningioma (n = 24), with an average age of 65.4 years, were included. The patients were classified into 2 groups, the homogeneous and heterogeneous groups, based on the contrast-enhanced T1-weighted MRI findings. Further, baseline demographics (age, sex, presence of preoperative paralysis [manual muscle testing 3 or worse neurological deficit in upper and/or lower limbs], tumor level, tumor length, and tumor occupation ratio), histological findings (Ki-67 index and histological subtypes), and CT findings (presence of intratumor calcification and Hounsfield unit [HU] value) were examined.
Preoperative paralysis was observed in 33.3% (8 of 24) of the patients. These patients exhibited frequent heterogeneous contrast-enhanced MRI findings than those without preoperative paralysis (57.1% vs. 14.3%, p = 0.040). Further, preoperative paralysis did not associate with tumor level, tumor length, tumor-occupied ratio, Ki-67 index, and histological subtypes. The heterogeneous group showed 100% intratumor calcification and higher maximum HU than the homogeneous group (1,109.8 vs. 379.2, p = 0.001).
The heterogeneous contrast-induced MRI findings in the spinal meningioma were significantly associated with preoperative neurological impairment. Moreover, the intratumor contrast-deficient region in the heterogeneously enhanced tumors reflected marked calcification. The tumor hardness due to calcification may be related to preoperative neurological deficit.
脊髓脑膜瘤大多为良性,但可出现神经功能缺损。神经功能损害与其影像学表现之间的关系,包括肿瘤内磁共振成像(MRI)钆增强和计算机断层扫描(CT)中的钙化,尚未得到研究。本研究的目的是探讨脊髓脑膜瘤术前影像表现与神经状态的相关性。
纳入组织学诊断为脊髓脑膜瘤的患者(n = 24),平均年龄65.4岁。根据对比增强T1加权MRI表现,将患者分为两组,即均匀组和不均匀组。此外,还检查了基线人口统计学特征(年龄、性别、术前瘫痪情况[上肢和/或下肢手动肌力测试为3级或更差的神经功能缺损]、肿瘤节段、肿瘤长度和肿瘤占位比)、组织学表现(Ki-67指数和组织学亚型)以及CT表现(肿瘤内钙化情况和亨氏单位[HU]值)。
33.3%(24例中的8例)的患者术前出现瘫痪。与无术前瘫痪的患者相比,这些患者的MRI对比增强表现不均匀的情况更为常见(57.1%对14.3%,p = 0.040)。此外,术前瘫痪与肿瘤节段、肿瘤长度、肿瘤占位比、Ki-67指数和组织学亚型无关。不均匀组的肿瘤内钙化率为100%,且最大HU值高于均匀组(1109.8对379.2,p = 0.001)。
脊髓脑膜瘤中不均匀的对比增强MRI表现与术前神经功能损害显著相关。此外,不均匀强化肿瘤内的对比剂缺乏区域反映了明显的钙化。钙化导致的肿瘤硬度可能与术前神经功能缺损有关。