Department of Radiotherapy, The Royal Marsden NHS Foundation Trust, London, UK.
Lungs for Living Research Centre, UCL Respiratory, Rayne Institute, University College London, London, UK.
Br J Cancer. 2020 Dec;123(Suppl 1):18-27. doi: 10.1038/s41416-020-01071-5.
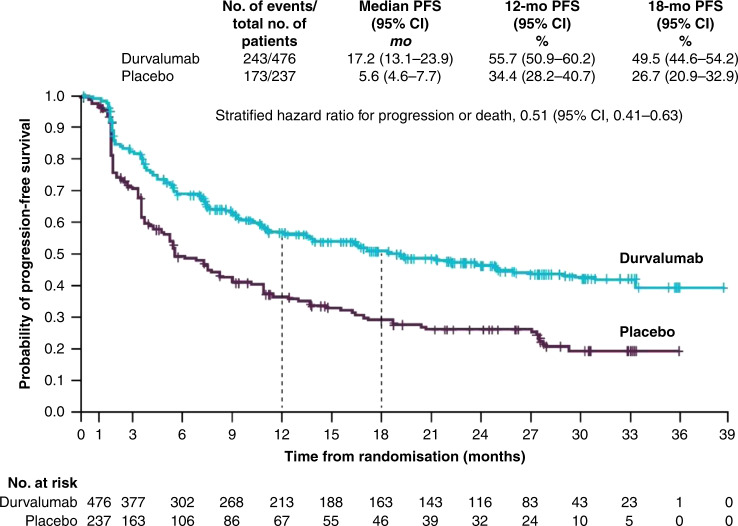
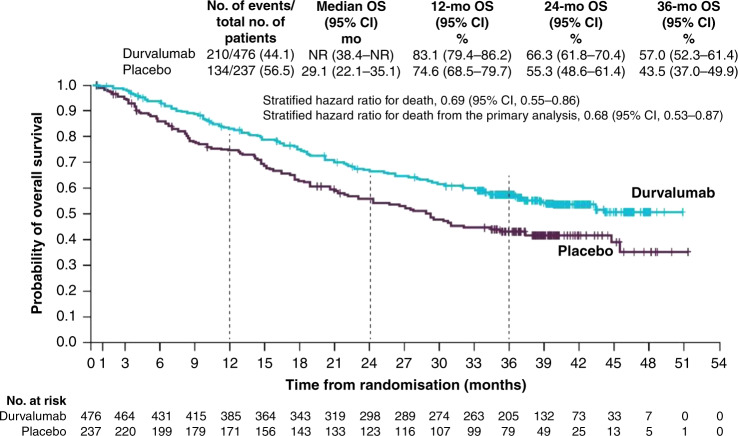
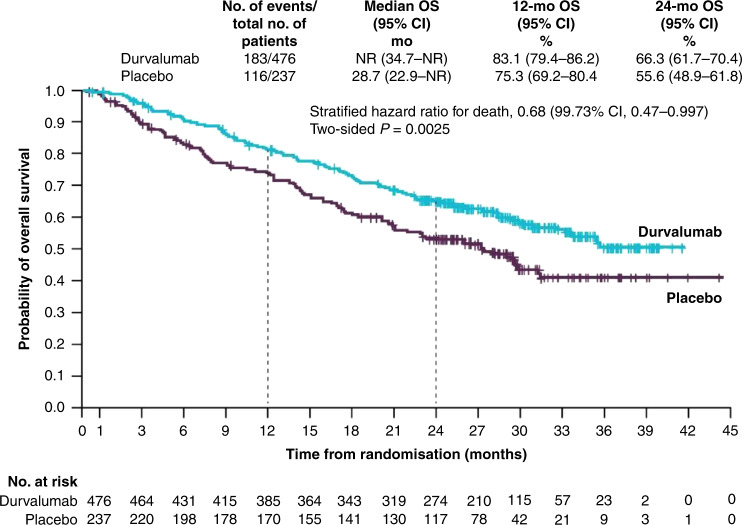
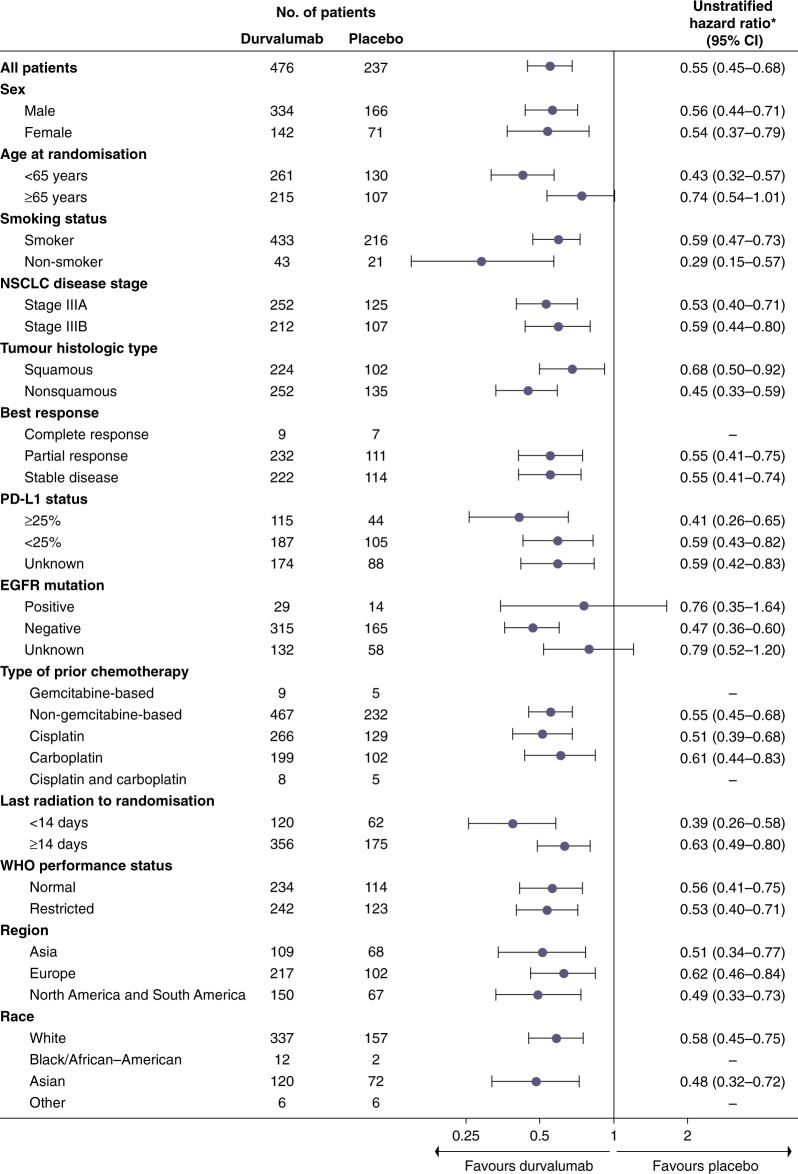
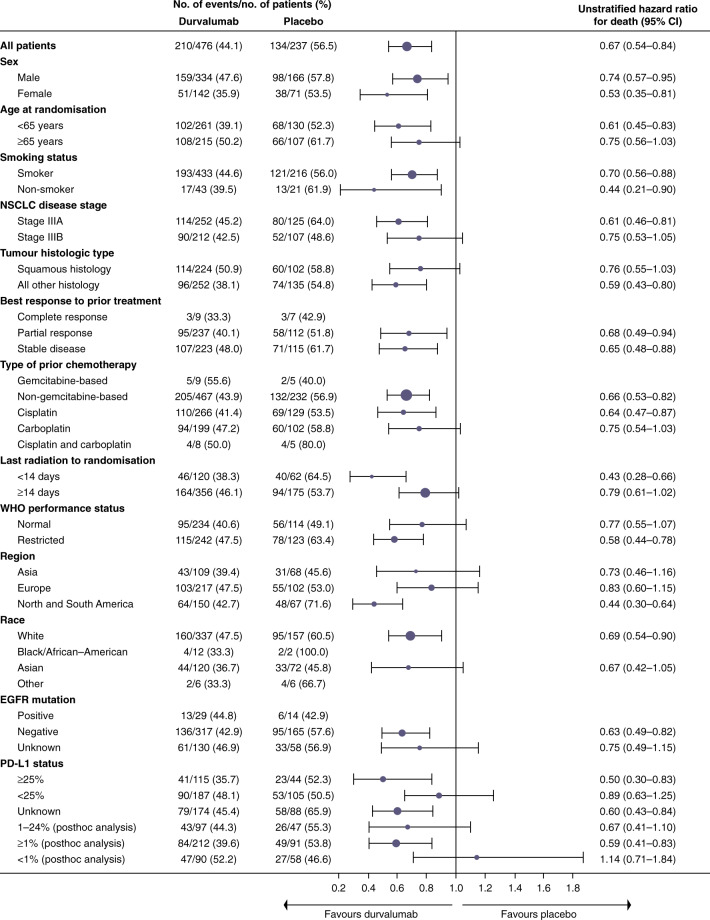
The treatment paradigm of non-small-cell lung cancer (NSCLC) has rapidly changed in recent years following the introduction of immune-checkpoint inhibition (ICI). Pre-clinically, both chemotherapy and radiotherapy modulate the tumour microenvironment, providing the rationale for clinical trials evaluating their role in combination with immunotherapy. Standard-of-care treatment for patients with unresectable stage III disease is concurrent chemoradiotherapy (cCRT); however, only recently, the combination with ICI has been explored. The Phase 3 PACIFIC study randomised 713 patients with confirmed locally advanced, unresectable, stage III NSCLC, whose disease has not progressed following cCRT, to either the anti-programmed death-ligand 1 (PD-L1) agent durvalumab (Imfinzi▼, AstraZeneca UK Limited) or placebo. Patients with a PD-L1 status ≥1% treated with durvalumab had a significantly longer median progression-free survival compared with placebo (17.2 vs. 5.6 months, respectively; HR: 0.51; 95% CI: 0.41-0.63), prolonged median overall survival (OS) (NR vs. 28.7 months, respectively; HR: 0.68; 99.73% CI: 0.47-0.997; P = 0.0025) and long-term clinical benefit (3-year OS HR: 0.69; 95% CI: 0.55-0.86). Grade 3 or 4 toxicity was marginally greater in the durvalumab cohort versus placebo (30.5% vs. 26.1%). Based on these results, durvalumab has been licensed in this setting, and further clinical trials are exploring the use of ICI in unresectable stage III NSCLC.
近年来,随着免疫检查点抑制(ICI)的引入,非小细胞肺癌(NSCLC)的治疗模式发生了迅速变化。在临床前研究中,化疗和放疗都可以调节肿瘤微环境,这为评估它们与免疫疗法联合应用的临床试验提供了依据。不可切除的 III 期疾病患者的标准治疗方法是同步放化疗(cCRT);然而,直到最近,ICI 的联合应用才得到探索。III 期 PACIFIC 研究将 713 名经确认的局部晚期、不可切除的 III 期 NSCLC 患者随机分组,这些患者在 cCRT 后疾病未进展,分别接受抗程序性死亡配体 1(PD-L1)药物度伐利尤单抗(Imfinzi▼,阿斯利康英国有限公司)或安慰剂治疗。接受度伐利尤单抗治疗且 PD-L1 状态≥1%的患者,与安慰剂相比,中位无进展生存期显著延长(分别为 17.2 个月 vs. 5.6 个月;HR:0.51;95%CI:0.41-0.63),中位总生存期(OS)延长(NR 与 28.7 个月,分别;HR:0.68;99.73%CI:0.47-0.997;P = 0.0025),并且长期临床获益(3 年 OS HR:0.69;95%CI:0.55-0.86)。度伐利尤单抗组与安慰剂组相比,3 级或 4 级毒性略有增加(30.5% vs. 26.1%)。基于这些结果,度伐利尤单抗已在该适应证中获得批准,并且进一步的临床试验正在探索免疫检查点抑制剂在不可切除的 III 期 NSCLC 中的应用。