Department of Quantitative Health Sciences, John A. Burns School of Medicine, University of Hawaii, 651 Ilalo Street, Medical Education Building, Suite 411, Honolulu, HI, 96813, USA.
Department of Family, Population & Preventive Medicine, Stony Brook University Medical Center, HSC L3, Rm 086, Stony Brook, NY, 11794-8036, USA.
Health Qual Life Outcomes. 2020 Dec 9;18(1):380. doi: 10.1186/s12955-020-01625-4.
This study examined racial/ethnic differences in health-related quality of life (HRQOL) among adults and identified variables associated with HRQOL by race/ethnicity.
This study was conducted under a cross-sectional design. We used the 2011-2016 Hawaii Behavioral Risk Factor Surveillance System data. HRQOL were assessed by four measures: self-rated general health, physically unhealthy days, mentally unhealthy days, and days with activity limitation. Distress was defined as fair/poor for general health and 14 days or more for each of the other three HRQOL measures. We conducted multivariable logistic regressions with variables guided by Anderson's behavioral model on each distress measure by race/ethnicity.
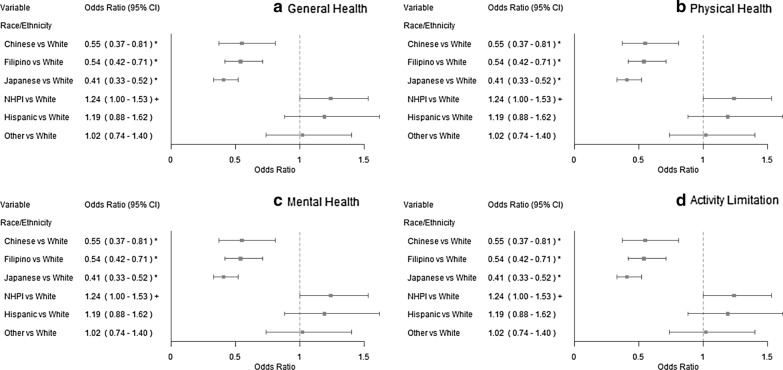
Among Hawaii adults, 30.4% were White, 20.9% Japanese, 16.8% Filipino, 14.6% Native Hawaiian and Pacific Islander (NHPI), 5.9% Chinese, 5.2% Hispanics, and 6.2% Other. We found significant racial/ethnic differences in the HRQOL measures. Compared to Whites, Filipinos, Japanese, NHPIs, and Hispanics showed higher distress rates in general health, while Filipinos and Japanese showed lower distress rates in the other HRQOL measures. Although no variables were consistently associated with all four HRQOL measures across all racial/ethnic groups, history of diabetes were significantly associated with general health across all racial/ethnic groups and history of depression was associated with at least three of the HRQOL measure across all racial/ethnic groups.
This study contributes to the literature on disparities in HRQOL and its association with other variables among diverse racial/ethnic subgroups. Knowing the common factors for HRQOL across different racial/ethnic groups and factors specific to different racial/ethnic groups will provide valuable information for identifying future public health priorities to improve quality of life and reduce health disparities.
本研究考察了成年人健康相关生活质量(HRQOL)的种族/民族差异,并确定了与 HRQOL 相关的种族/民族差异变量。
本研究采用横断面设计。我们使用了 2011-2016 年夏威夷行为风险因素监测系统的数据。HRQOL 通过四项指标进行评估:自我评估总体健康状况、身体不健康天数、心理不健康天数和活动受限天数。将一般健康状况的“一般/较差”和其他三项 HRQOL 指标中任何一项的 14 天或以上定义为“苦恼”。我们根据安德森行为模式,对每个苦恼指标进行了多变量逻辑回归分析,以种族/民族为导向。
在夏威夷成年人中,30.4%为白人,20.9%为日本人,16.8%为菲律宾人,14.6%为夏威夷原住民和太平洋岛民(NHPI),5.9%为中国人,5.2%为西班牙裔,6.2%为其他族裔。我们发现,在 HRQOL 指标方面存在显著的种族/民族差异。与白人相比,菲律宾人、日本人、NHPI 和西班牙裔的一般健康状况苦恼率较高,而菲律宾人和日本人在其他 HRQOL 指标上的苦恼率较低。虽然在所有种族/民族群体中,没有一个变量与所有四项 HRQOL 指标都始终相关,但糖尿病史与所有种族/民族群体的总体健康状况显著相关,而抑郁症史与所有种族/民族群体的至少三项 HRQOL 指标相关。
本研究为不同种族/民族亚组的 HRQOL 差异及其与其他变量的关联研究做出了贡献。了解不同种族/民族群体之间 HRQOL 的共同因素和特定于不同种族/民族群体的因素,将为确定未来的公共卫生重点提供有价值的信息,以提高生活质量,减少健康差距。