UT Southwestern Medical School.
UT Southwestern Health Sciences Digital Library and Learning Center.
Cancer J. 2020 Nov/Dec;26(6):525-536. doi: 10.1097/PPO.0000000000000484.
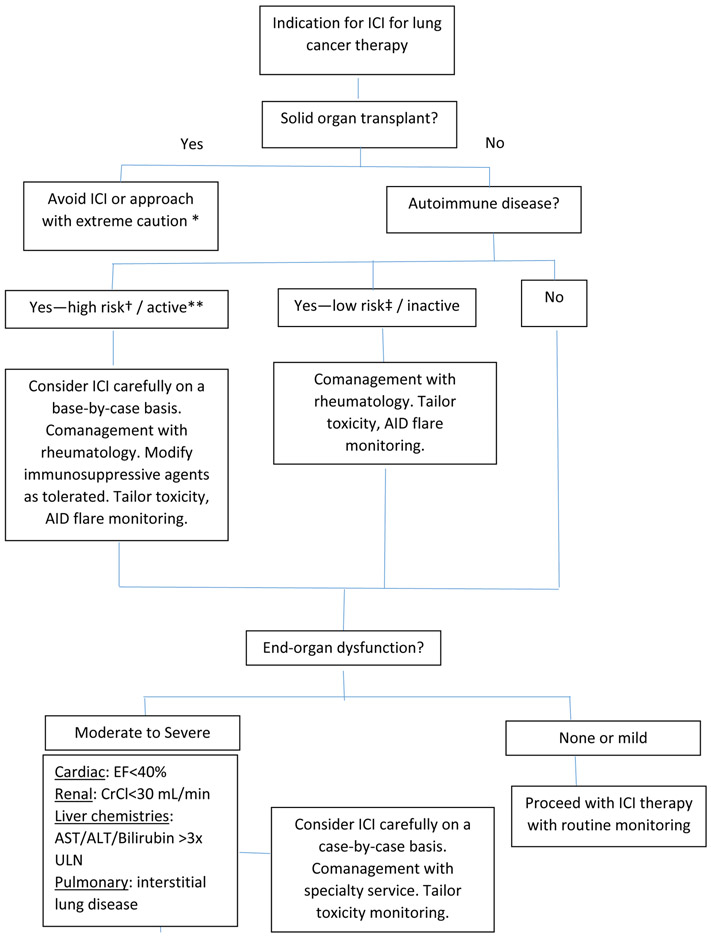
Immune checkpoint inhibitor (ICI) therapy is now in widespread clinical use for the treatment of lung cancer. Although patients with autoimmune disease and other comorbidities were excluded from initial clinical trials, emerging real-world experience suggests that these promising treatments may be administered safely to individuals with inactive low-risk autoimmune disease such as rheumatoid arthritis or psoriasis, mild to moderate renal and hepatic dysfunction, and certain chronic viral infections. Considerations for ICI in autoimmune disease populations include exacerbations of the underlying autoimmune disease, increased risk of ICI-induced immune-related adverse events, and potential for compromised efficacy if patients are receiving chronic immunosuppression. Immune checkpoint inhibitor use in higher-risk autoimmune conditions, such as myasthenia gravis or multiple sclerosis, requires careful evaluation on a case-by-case basis. Immune checkpoint inhibitor use in individuals with solid organ transplant carries a substantial risk of organ rejection. Ongoing research into the prediction of ICI efficacy and toxicity may help in patient selection, treatment, and monitoring.
免疫检查点抑制剂 (ICI) 治疗现已广泛应用于肺癌的临床治疗。尽管最初的临床试验排除了自身免疫性疾病和其他合并症患者,但新兴的实际经验表明,这些有前途的治疗方法可能安全地应用于患有不活跃的低风险自身免疫性疾病的个体,如类风湿关节炎或银屑病、轻度至中度肾功能和肝功能障碍,以及某些慢性病毒感染。在自身免疫性疾病人群中使用 ICI 时需要考虑的因素包括基础自身免疫性疾病的加重、ICI 诱导的免疫相关不良事件风险增加,以及如果患者正在接受慢性免疫抑制治疗,疗效可能受到影响的潜在风险。在患有重症肌无力或多发性硬化症等高危自身免疫性疾病的人群中使用免疫检查点抑制剂需要逐案进行仔细评估。在实体器官移植受者中使用免疫检查点抑制剂会带来器官排斥的巨大风险。目前正在进行的关于 ICI 疗效和毒性预测的研究可能有助于患者选择、治疗和监测。