Liu Kevin X, Chen Yu-Hui, Kozono David, Mak Raymond H, Boyle Patrick J, Janeway Katherine A, Mullen Elizabeth A, Marcus Karen J
Department of Radiation Oncology, Brigham and Women's Hospital, Dana-Farber Cancer Institute, Boston Children's Hospital, Harvard Medical School, Boston, Massachusetts.
Department of Data Sciences, Dana-Farber Cancer Institute, Boston, Massachusetts.
Adv Radiat Oncol. 2020 Sep 23;5(6):1267-1273. doi: 10.1016/j.adro.2020.09.004. eCollection 2020 Nov-Dec.
Pulmonary metastases are common in many pediatric solid tumors; however, little is known about safety and efficacy of lung stereotactic body radiation therapy (SBRT) for pediatric patients. We conducted a phase I/II study to investigate the minimum effective dose level of SBRT with an acceptable safety profile in pediatric patients.
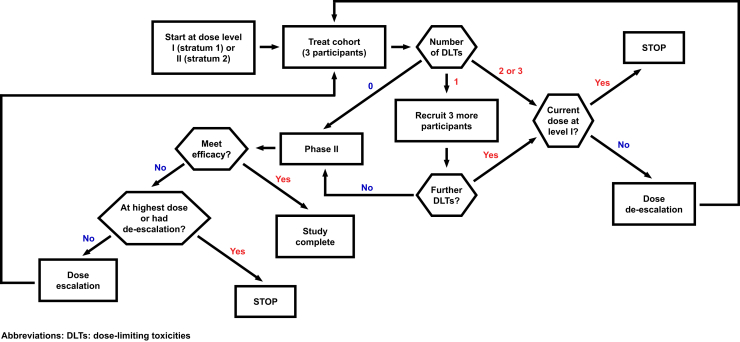
Patients with sarcoma and metastatic pulmonary lesions ≤3 cm in diameter and ≤21 years of age were enrolled. Dose levels 1, 2, and 3 were 24, 30, and 36 Gy in 3 fractions, respectively. Enrolled patients with metastases from primary renal tumors and sarcoma histologies were to begin at dose level 1 and 2, respectively. Exclusion criteria included receipt of whole-lung/hemi-thorax irradiation >12 Gy within 6 months of consent. Primary endpoints were tolerability and safety per Common Terminology Criteria for Adverse Events grading and disease response at 6 weeks post-SBRT per response evaluation criteria in solid tumors (RECIST) 1.1 criteria. Secondary endpoints included rates of local control and distant failure within the lung, but outside of the treatment volume.
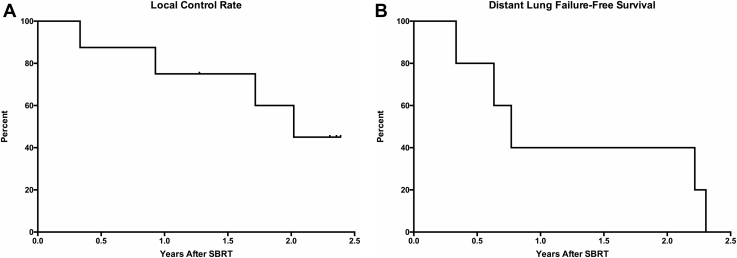
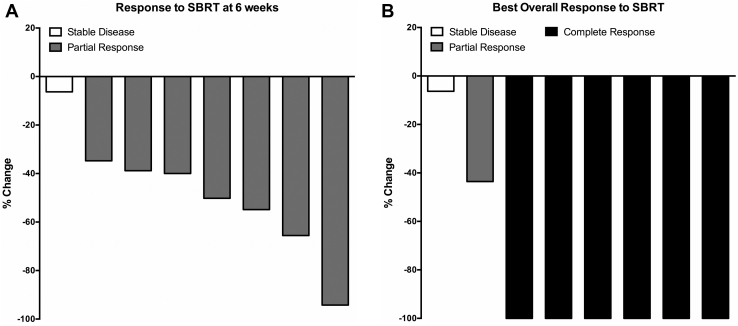
Five patients with median age of 13 years (range, 7-21) received SBRT at dose level 2. Primary tumor histologies included Ewing sarcoma (n = 3), anaplastic chordoma (n = 1), and osteosarcoma (n = 1). No grade ≥3 adverse events were observed. At 6 weeks after SBRT, 7/8 (87.5%) lesions achieved partial response. With median follow-up of 2.1 years (range, 1.4-2.5), 2-year local control and distant failure-free survival were 60% (n = 8) and 40% (n = 5), respectively. One patient developed widespread metastases and succumbed to disease 1.4 years after SBRT.
SBRT for pulmonary metastases produces responses in pediatric patients with sarcoma at 6 weeks with acceptable toxicity; however, patients remain at risk of local and distant failure within the lung. Future prospective studies are needed to investigate whether higher doses of SBRT, possibly in combination with other therapies, are safe and provide more durable response.
肺转移在许多小儿实体瘤中很常见;然而,对于小儿患者的肺部立体定向体部放射治疗(SBRT)的安全性和有效性知之甚少。我们开展了一项I/II期研究,以调查在小儿患者中具有可接受安全性的SBRT的最小有效剂量水平。
纳入直径≤3 cm且年龄≤21岁的肉瘤和肺转移病变患者。剂量水平1、2和3分别为24、30和36 Gy,分3次给予。纳入的原发性肾肿瘤转移患者和肉瘤组织学患者分别从剂量水平1和2开始。排除标准包括在签署知情同意书后6个月内接受全肺/半胸照射>12 Gy。主要终点是根据不良事件通用术语标准分级的耐受性和安全性,以及根据实体瘤疗效评价标准(RECIST)1.1标准在SBRT后6周的疾病反应。次要终点包括肺部局部控制率和远处失败率,但不包括治疗体积内。
5例中位年龄为13岁(范围7 - 21岁)的患者接受了剂量水平2的SBRT。原发性肿瘤组织学类型包括尤因肉瘤(n = 3)、间变性脊索瘤(n = 1)和骨肉瘤(n = 1)。未观察到≥3级不良事件。SBRT后6周,7/8(87.5%)的病变达到部分缓解。中位随访2.1年(范围1.4 - 2.5年),2年局部控制率和无远处失败生存率分别为60%(n = 8)和40%(n = 5)。1例患者出现广泛转移,并在SBRT后1.4年死于疾病。
SBRT治疗小儿肉瘤肺转移在6周时产生反应,毒性可接受;然而,患者仍有肺部局部和远处失败的风险。未来需要进行前瞻性研究,以调查更高剂量的SBRT,可能与其他疗法联合使用,是否安全并能提供更持久的反应。