Division of Brain, Imaging, and Behaviour-Systems Neuroscience, Krembil Research Institute, Toronto Western Hospital, University Health Network, Toronto, ON, Canada.
Institute of Medical Science, Faculty of Medicine, University of Toronto, Toronto, ON, Canada.
Pain. 2021 Jun 1;162(6):1790-1799. doi: 10.1097/j.pain.0000000000002164.
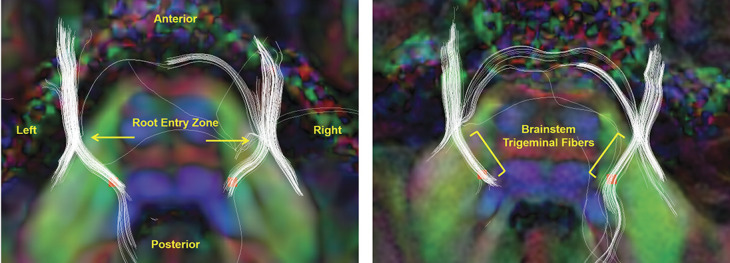
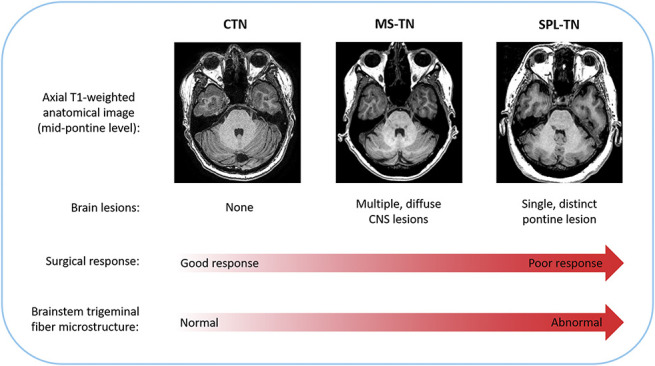
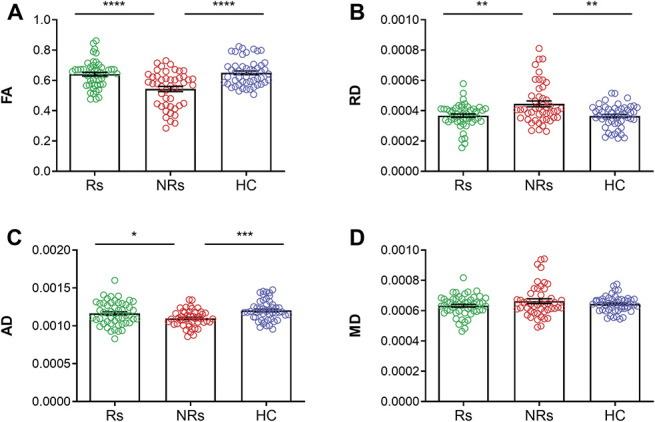
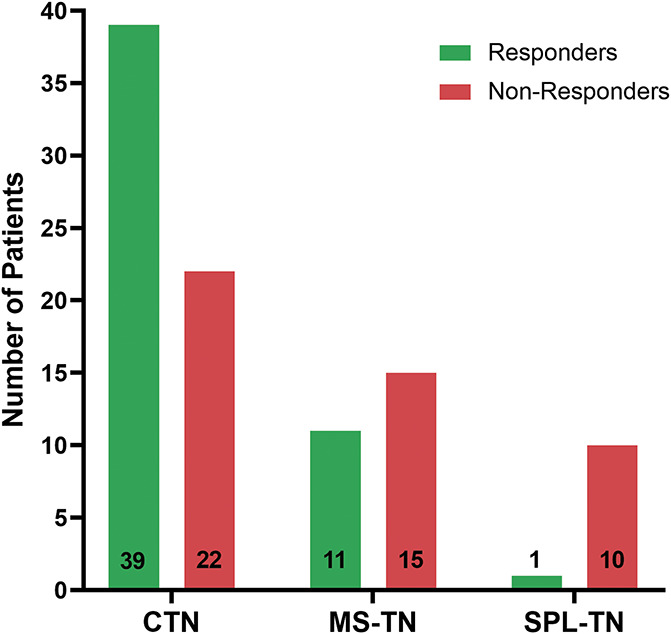
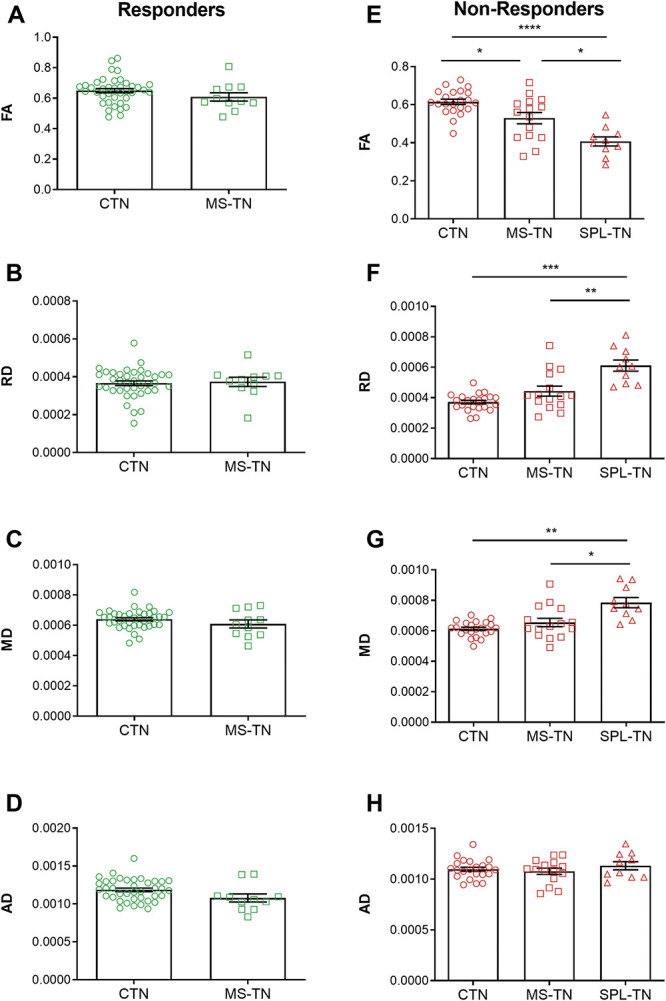
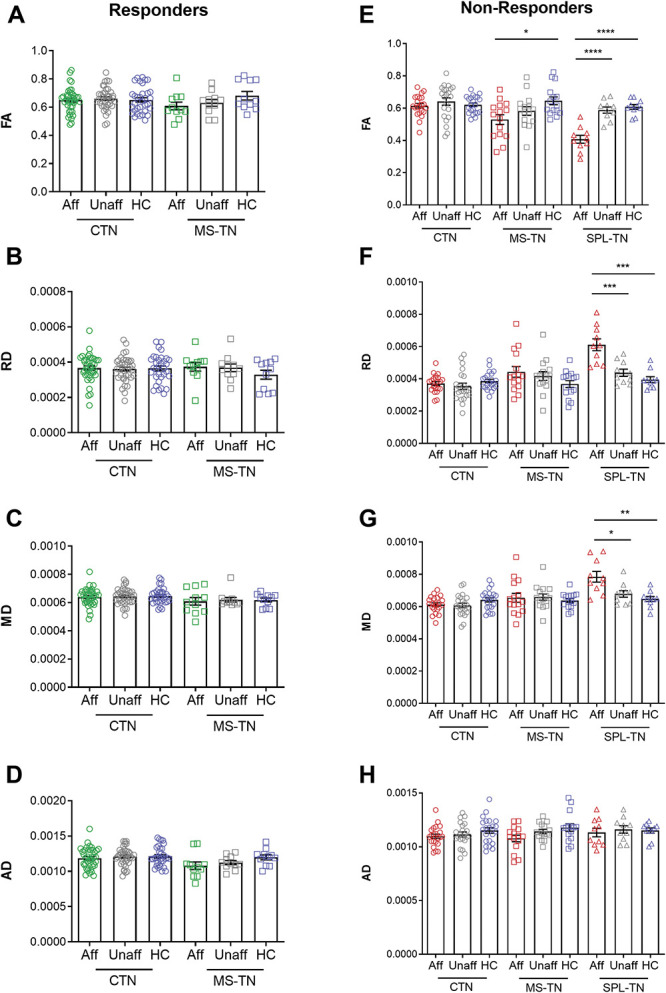
Neurosurgical treatments for trigeminal neuralgia (TN) can provide long-lasting pain relief; however, some patients fail to respond and undergo multiple, repeat procedures. Surgical outcomes can vary depending on the type of TN, but the reasons for this are not well understood. Neuroimaging studies of TN point to abnormalities in the brainstem trigeminal fibers; however, whether this is a common characteristic of treatment nonresponse across different subtypes of TN is unknown. Here, we used diffusion tensor imaging (DTI) to determine whether the brainstem trigeminal fiber microstructure is a common biomarker of surgical response in TN and whether the extent of these abnormalities is associated with the likelihood of response across subtypes of TN. We studied 98 patients with TN (61 classical TN, 26 TN secondary to multiple sclerosis, and 11 TN associated with a solitary pontine lesion) who underwent neurosurgical treatment and 50 healthy controls. We assessed treatment response using pain intensity measures and examined microstructural features by extracting pretreatment DTI metrics from the proximal pontine segment of the trigeminal nerves. We found that microstructural abnormalities in the affected pontine trigeminal fibers (notably, lower fractional anisotropy and higher radial diffusivity) highlight treatment nonresponders (n = 47) compared with responders (n = 51) and controls, and that the degree of abnormalities is associated with the likelihood of surgical response across subtypes of TN. These novel findings demonstrate the value of DTI as an objective, noninvasive tool for the prediction of treatment response and elucidate the features that distinguish treatment responders from nonresponders in the TN population.
神经外科治疗三叉神经痛 (TN) 可以提供持久的疼痛缓解;然而,一些患者对治疗没有反应,并接受了多次重复手术。手术结果可能因 TN 的类型而异,但原因尚不清楚。TN 的神经影像学研究表明脑干三叉神经纤维存在异常;然而,这种异常是否是不同亚型 TN 治疗无反应的共同特征尚不清楚。在这里,我们使用弥散张量成像 (DTI) 来确定脑干三叉神经纤维微观结构是否是 TN 手术反应的共同生物标志物,以及这些异常的程度是否与不同亚型 TN 的反应可能性相关。我们研究了 98 例接受神经外科治疗的 TN 患者(61 例经典 TN、26 例多发性硬化症继发 TN 和 11 例与孤立性脑桥病变相关的 TN)和 50 名健康对照者。我们使用疼痛强度测量来评估治疗反应,并通过从三叉神经的近端桥脑段提取预处理 DTI 指标来检查微观结构特征。我们发现,受影响的桥脑三叉神经纤维的微观结构异常(特别是较低的各向异性分数和较高的径向扩散系数)突出了治疗无反应者(n = 47)与反应者(n = 51)和对照组之间的差异,并且异常程度与不同亚型 TN 的手术反应可能性相关。这些新发现表明 DTI 作为一种客观、非侵入性的工具,可用于预测治疗反应,并阐明了 TN 人群中区分治疗反应者和无反应者的特征。