Martellucci Salvatore, Malara Pasquale, Castellucci Andrea, Pecci Rudi, Giannoni Beatrice, Marcelli Vincenzo, Scarpa Alfonso, Cassandro Ettore, Quaglieri Silvia, Manfrin Marco Lucio, Rebecchi Elisabetta, Armato Enrico, Comacchio Francesco, Mion Marta, Attanasio Giuseppe, Ralli Massimo, Greco Antonio, de Vincentiis Marco, Botti Cecilia, Savoldi Luisa, Califano Luigi, Ghidini Angelo, Pagliuca Giulio, Clemenzi Veronica, Stolfa Andrea, Gallo Andrea, Asprella Libonati Giacinto
ENT Unit, Santa Maria Goretti Hospital, AUSL Latina, Latina, Italy.
Audiology & Vestibology Service, Centromedico Bellinzona, Bellinzona, Switzerland.
Front Neurol. 2020 Nov 19;11:578305. doi: 10.3389/fneur.2020.578305. eCollection 2020.
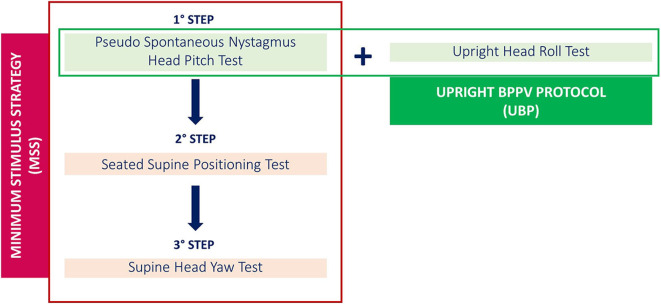
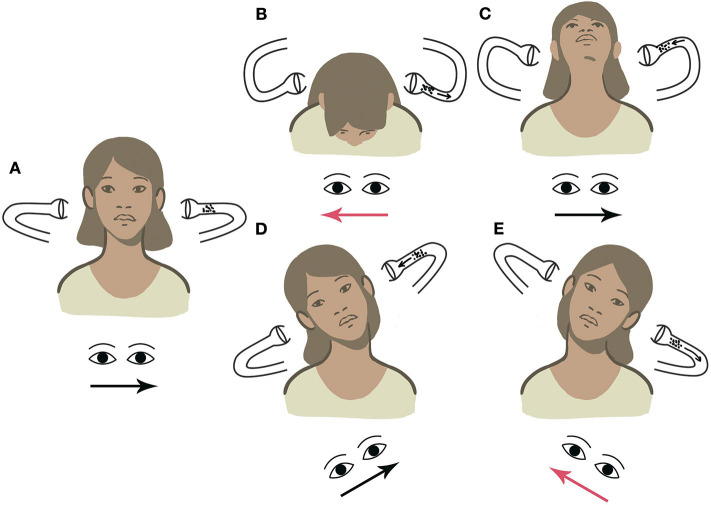
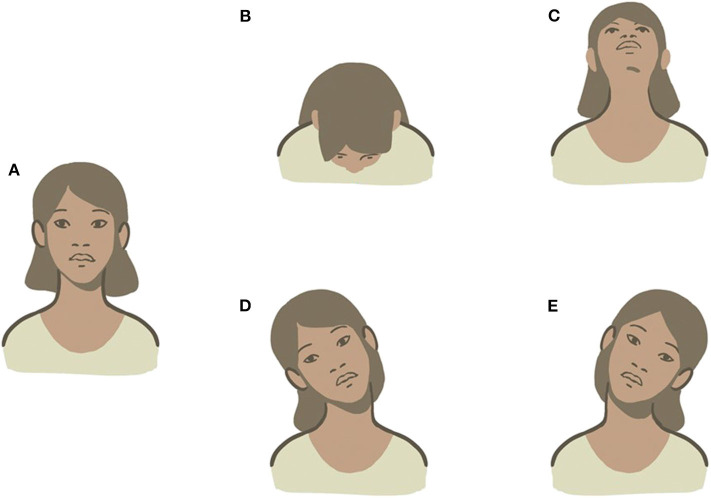
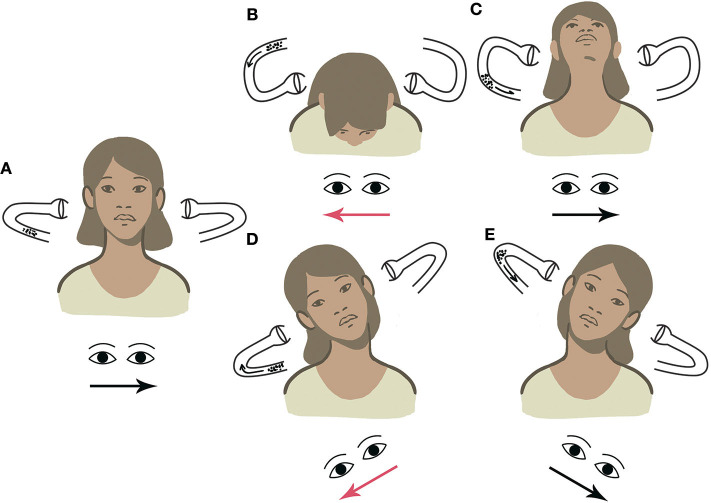
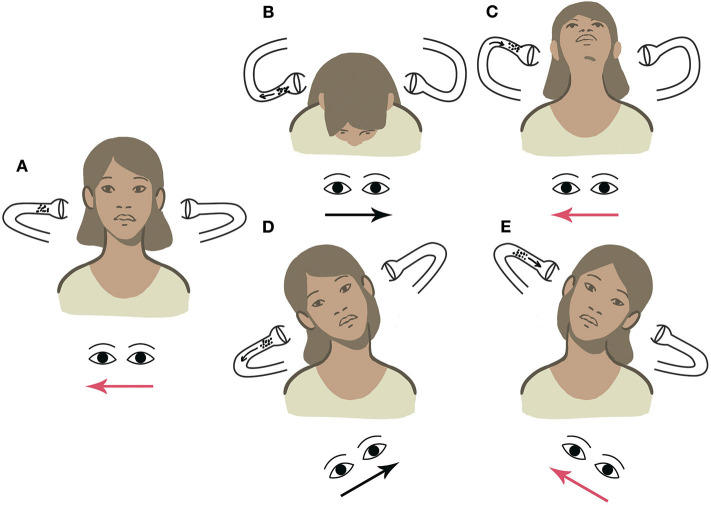
The diagnosis of benign paroxysmal positional vertigo (BPPV) involving the lateral semicircular canal (LSC) is traditionally entrusted to the supine head roll test, also known as supine head yaw test (SHYT), which usually allows identification of the pathologic side and BPPV form (geotropic vs. apogeotropic). Nevertheless, SHYT may not always allow easy detection of the affected canal, resulting in similar responses on both sides and intense autonomic symptoms in patients with recent onset of vertigo. The newly introduced upright head roll test (UHRT) represents a diagnostic maneuver for LSC-BPPV, supplementing the already-known head pitch test (HPT) in the sitting position. The combination of these two tests should enable clinicians to determine the precise location of debris within LSC, avoiding disturbing symptoms related to supine positionings. Therefore, we proposed the upright BPPV protocol (UBP), a test battery exclusively performed in the upright position, including the evaluation of pseudo-spontaneous nystagmus (PSN), HPT and UHRT. The purpose of this multicenter study is to determine the feasibility of UBP in the diagnosis of LSC-BPPV. We retrospectively reviewed the clinical data of 134 consecutive patients diagnosed with LSC-BPPV. All of them received both UBP and the complete diagnostic protocol (CDP), including the evaluation of PSN and data resulting from HPT, UHRT, seated-supine positioning test (SSPT), and SHYT. A correct diagnosis for LSC-BPPV was achieved in 95.5% of cases using exclusively the UBP, with a highly significant concordance with the CDP ( < 0.000, Cohen's kappa = 0.94), regardless of the time elapsed from symptom onset to diagnosis. The concordance between UBP and CDP was not impaired even when cases in which HPT and/or UHRT provided incomplete results were included ( < 0.000). Correct diagnosis using the supine diagnostic protocol (SDP, including SSPT + SHYT) or the sole SHYT was achieved in 85.1% of cases, with similar statistical concordance ( < 0.000) and weaker strength of relationship (Cohen's kappa = 0.80). UBP allows correct diagnosis in LSC-BPPV from the sitting position in most cases, sparing the patient supine positionings and related symptoms. UBP could also allow clinicians to proceed directly with repositioning maneuvers from the upright position.
涉及外侧半规管(LSC)的良性阵发性位置性眩晕(BPPV)的诊断传统上依靠仰卧位摇头试验,也称为仰卧位头部偏航试验(SHYT),该试验通常能够确定患侧及BPPV的类型(地向性与背地性)。然而,SHYT可能并不总能轻易检测出受累的半规管,导致两侧反应相似,且近期发作眩晕的患者会出现强烈的自主神经症状。新引入的直立位摇头试验(UHRT)是一种针对LSC-BPPV的诊断手法,它补充了已为人知的坐位头部俯仰试验(HPT)。这两种试验的联合应用应能使临床医生确定LSC内耳石碎片的精确位置,避免与仰卧位相关的不适症状。因此,我们提出了直立位BPPV方案(UBP),这是一种仅在直立位进行的试验组合,包括对假性自发性眼震(PSN)、HPT和UHRT的评估。这项多中心研究的目的是确定UBP在诊断LSC-BPPV中的可行性。我们回顾性分析了134例连续诊断为LSC-BPPV患者的临床资料。所有患者均接受了UBP和完整诊断方案(CDP),后者包括对PSN的评估以及HPT、UHRT、坐卧体位试验(SSPT)和SHYT所得到的数据。仅使用UBP时,95.5%的病例实现了对LSC-BPPV的正确诊断,与CDP具有高度显著的一致性(<0.000,Cohen卡方值=0.94),无论从症状发作到诊断所经过的时间长短。即使纳入HPT和/或UHRT结果不完整的病例,UBP与CDP之间的一致性也未受影响(<0.000)。使用仰卧位诊断方案(SDP,包括SSPT+SHYT)或仅使用SHYT时,85.1%的病例实现了正确诊断,具有相似的统计学一致性(<0.000),但关联强度较弱(Cohen卡方值=0.80)。在大多数情况下,UBP能够从坐位对LSC-BPPV做出正确诊断,使患者免受仰卧位及相关症状之苦。UBP还可使临床医生直接从直立位进行复位手法操作。