Department of Obstetrics and Gynecology, Academic Hospital Paramaribo, Paramaribo, Suriname, South Africa.
Division Women and Baby, Department of Obstetrics, Birth Centre Wilhelmina's Children Hospital, University Medical Center Utrecht, Utrecht University, Utrecht, The Netherlands.
PLoS One. 2020 Dec 18;15(12):e0244087. doi: 10.1371/journal.pone.0244087. eCollection 2020.
Postpartum hemorrhage (PPH) is the leading cause of direct maternal mortality globally and in Suriname. We aimed to study the prevalence, risk indicators, causes, and management of PPH to identify opportunities for PPH reduction.
A nationwide retrospective descriptive study of all hospital deliveries in Suriname in 2017 was performed. Logistic regression analysis was applied to identify risk indicators for PPH (≥ 500ml blood loss). Management of severe PPH (blood loss ≥1,000ml or ≥500ml with hypotension or at least three transfusions) was evaluated via a criteria-based audit using the national guideline.
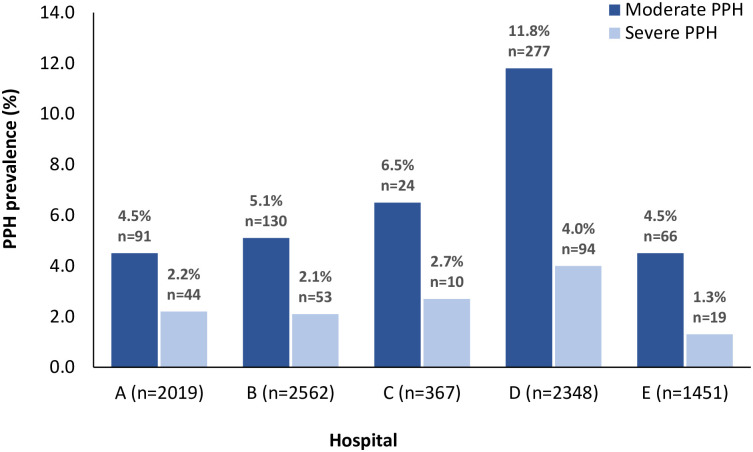
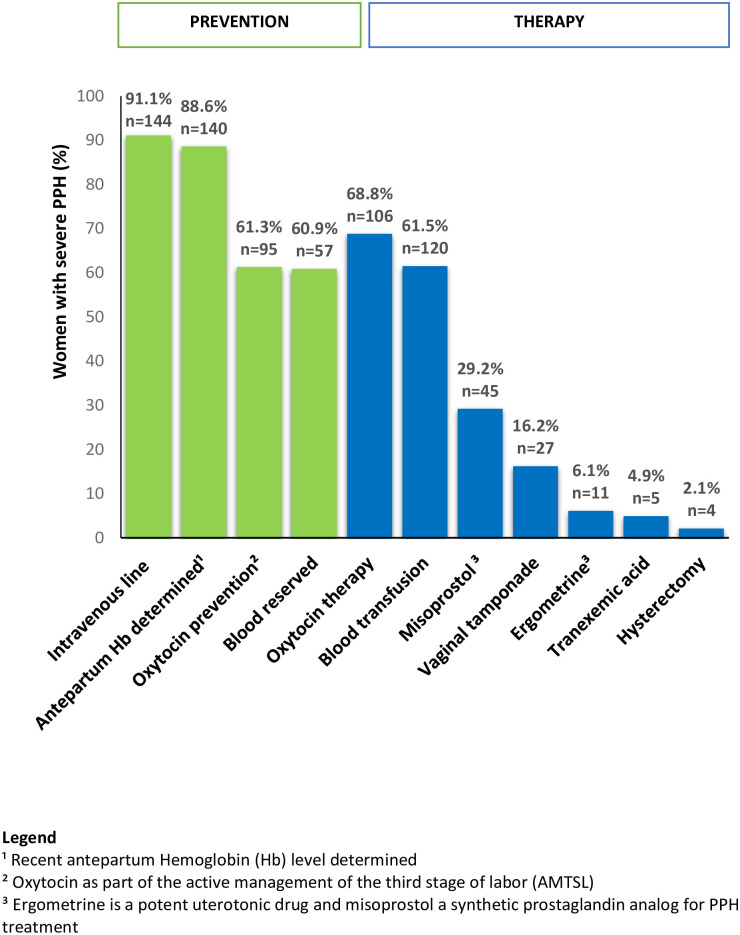
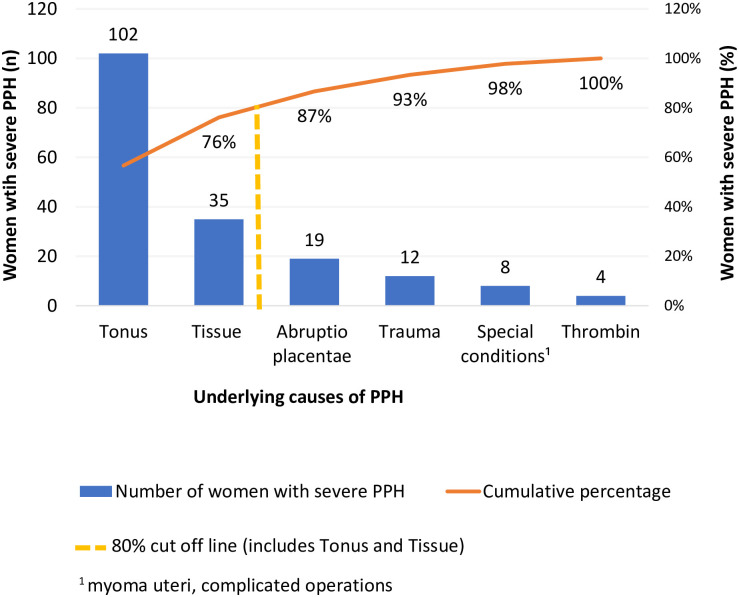
In 2017, the prevalence of PPH and severe PPH in Suriname was 9.2% (n = 808/8,747) and 2.5% (n = 220/8,747), respectively. PPH varied from 5.8% to 15.8% across the hospitals. Risk indicators associated with severe PPH included being of African descent (Maroon aOR 2.1[95%CI 1.3-3.3], Creole aOR 1.8[95%CI 1.1-3.0]), multiple pregnancy (aOR 3.4[95%CI 1.7-7.1]), delivery in Hospital D (aOR 2.4[95%CI 1.7-3.4]), cesarean section (aOR 3.9[95%CI 2.9-5.3]), stillbirth (aOR 6.4 [95%CI 3.4-12.2]), preterm birth (aOR 2.1[95%CI 1.3-3.2]), and macrosomia (aOR 2.8 [95%CI 1.5-5.0]). Uterine atony (56.7%, n = 102/180[missing 40]) and retained placenta (19.4%, n = 35/180[missing 40]), were the main causes of severe PPH. A criteria-based audit revealed that women with severe PPH received prophylactic oxytocin in 61.3% (n = 95/155[missing 65]), oxytocin treatment in 68.8% (n = 106/154[missing 66]), and tranexamic acid in 4.9% (n = 5/103[missing 117]).
PPH prevalence and risk indicators in Suriname were similar to international and regional reports. Inconsistent blood loss measurement, varied maternal and perinatal characteristics, and variable guideline adherence contributed to interhospital prevalence variation. PPH reduction in Suriname can be achieved through prevention by practicing active management of the third stage of labor in every birth and considering risk factors, early recognition by objective and consistent blood loss measurement, and prompt treatment by adequate administration of oxytocin and tranexamic acid according to national guidelines.
产后出血(PPH)是全球和苏里南产妇死亡的主要原因。我们旨在研究 PPH 的流行率、风险指标、原因和管理,以确定减少 PPH 的机会。
对 2017 年苏里南所有医院分娩进行全国性回顾性描述性研究。应用逻辑回归分析确定 PPH(≥500ml 失血)的风险指标。使用国家指南,通过基于标准的审核评估严重 PPH(失血≥1000ml 或≥500ml 伴低血压或至少三次输血)的管理。
2017 年,苏里南 PPH 和严重 PPH 的患病率分别为 9.2%(n=808/8747)和 2.5%(n=220/8747)。PPH 各医院间的差异从 5.8%到 15.8%不等。与严重 PPH 相关的风险指标包括非洲裔(马隆 aOR 2.1[95%CI 1.3-3.3],克里奥尔语 aOR 1.8[95%CI 1.1-3.0])、多胎妊娠(aOR 3.4[95%CI 1.7-7.1])、在医院 D 分娩(aOR 2.4[95%CI 1.7-3.4])、剖宫产(aOR 3.9[95%CI 2.9-5.3])、死产(aOR 6.4 [95%CI 3.4-12.2])、早产(aOR 2.1[95%CI 1.3-3.2])和巨大儿(aOR 2.8 [95%CI 1.5-5.0])。子宫收缩乏力(56.7%,n=102/180[缺失 40])和胎盘滞留(19.4%,n=35/180[缺失 40])是严重 PPH 的主要原因。基于标准的审核显示,严重 PPH 患者中,预防性使用催产素的比例为 61.3%(n=95/155[缺失 65]),催产素治疗的比例为 68.8%(n=106/154[缺失 66]),氨甲环酸的比例为 4.9%(n=5/103[缺失 117])。
苏里南的 PPH 患病率和风险指标与国际和地区报告相似。失血量测量不一致、母婴围产期特征差异以及指南遵循情况差异导致了各医院间患病率的差异。苏里南可以通过以下方式减少 PPH:通过在每次分娩中积极管理第三产程,考虑风险因素进行预防;通过客观和一致的失血量测量,早期识别;并根据国家指南,及时给予催产素和氨甲环酸充分治疗。