Oxford University Clinical Research Unit, Hospital for Tropical Diseases, Ho Chi Minh City, Vietnam.
University of Medicine and Pharmacy at Ho Chi Minh City, Ho Chi Minh City, Vietnam.
Clin Infect Dis. 2021 Jun 15;72(12):e1074-e1083. doi: 10.1093/cid/ciaa1840.
One of the generally accepted constructs of dengue pathogenesis is that clinical disease severity is at least partially dependent upon plasma viremia, yet data on plasma viremia in primary versus secondary infections and in relation to clinically relevant endpoints remain limited and contradictory.
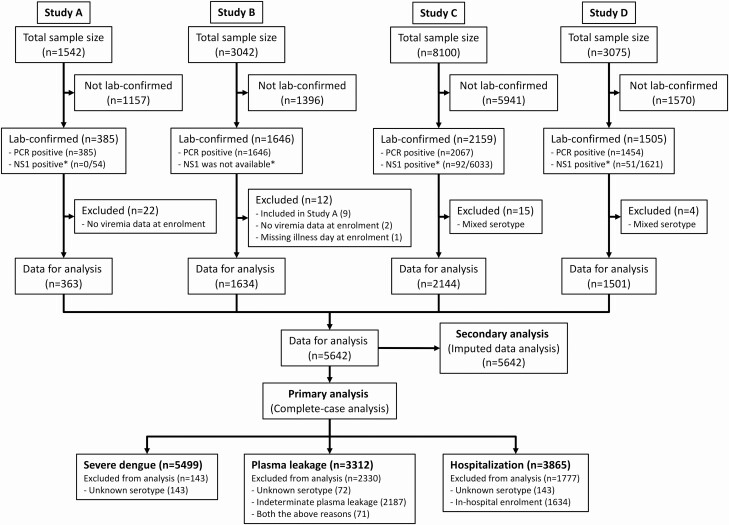
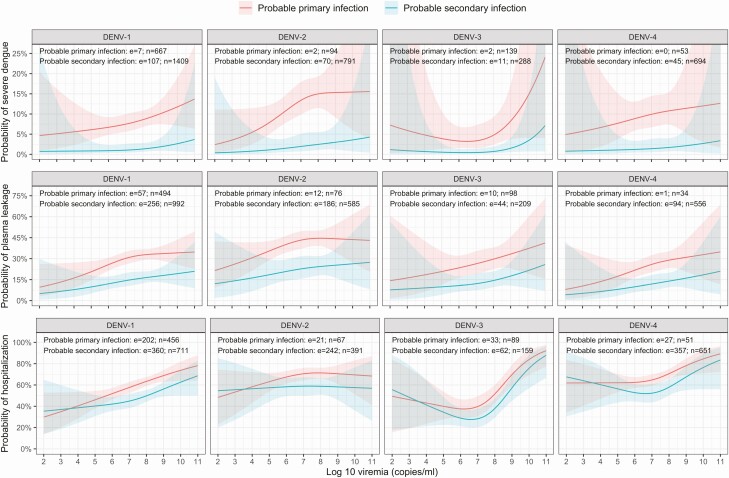
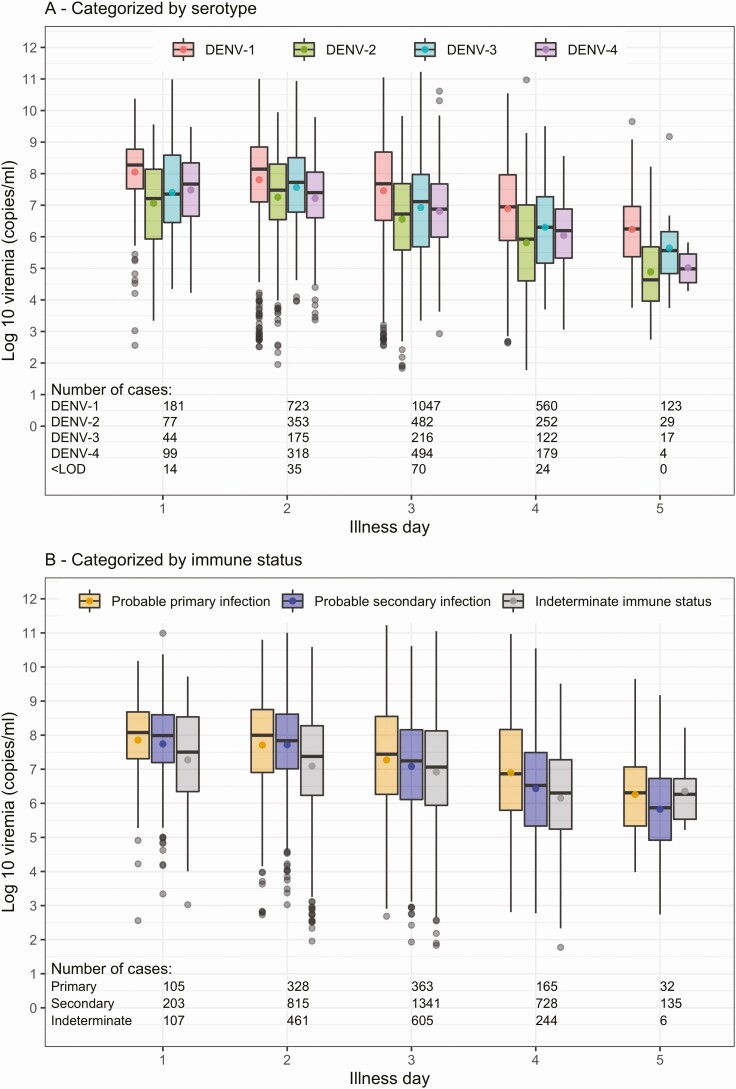
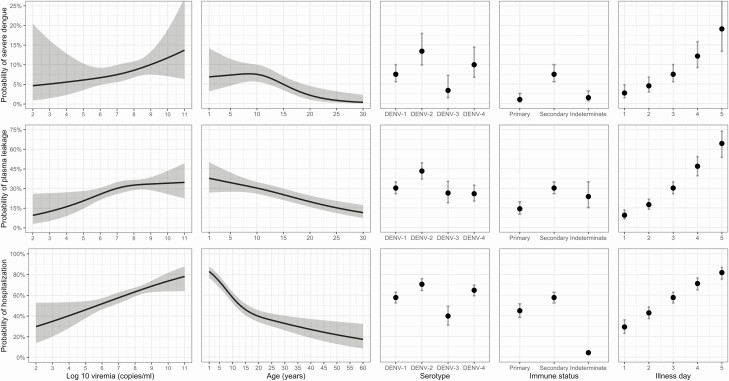
Using a large database comprising detailed clinical and laboratory characterization of Vietnamese participants enrolled in a series of research studies executed over a 15-year period, we explored relationships between plasma viremia measured by reverse transcription-polymerase chain reaction and 3 clinically relevant endpoints-severe dengue, plasma leakage, and hospitalization-in the dengue-confirmed cases. All 4 dengue serotypes and both primary and secondary infections were well represented. In our logistic regression models we allowed for a nonlinear effect of viremia and for associations between viremia and outcome to differ by age, serotype, host immune status, and illness day at study enrollment.
Among 5642 dengue-confirmed cases we identified 259 (4.6%) severe dengue cases, 701 (12.4%) patients with plasma leakage, and 1441 of 4008 (40.0%) patients recruited in outpatient settings who were subsequently hospitalized. From the early febrile phase onwards, higher viremia increased the risk of developing all 3 endpoints, but effect sizes were modest (ORs ranging from 1.12-1.27 per 1-log increase) compared with the effects of a secondary immune response (ORs, 1.67-7.76). The associations were consistent across age, serotype, and immune status groups, and in the various sensitivity and subgroup analyses we undertook.
Higher plasma viremia is associated with increased dengue severity, regardless of serotype or immune status.
登革热发病机制的公认构建之一是临床疾病严重程度至少部分取决于血浆病毒血症,但关于原发性和继发性感染以及与临床相关终点的血浆病毒血症的数据仍然有限且相互矛盾。
利用一个大型数据库,该数据库包含了在过去 15 年期间进行的一系列研究中登记的越南参与者的详细临床和实验室特征,我们探讨了通过逆转录-聚合酶链反应测量的血浆病毒血症与 3 个临床相关终点(重症登革热、血浆渗漏和住院)之间的关系,在确诊的登革热病例中。所有 4 种登革热血清型和原发性及继发性感染均有很好的代表性。在我们的逻辑回归模型中,我们允许病毒血症的非线性效应,并允许病毒血症与结局之间的关联因年龄、血清型、宿主免疫状态和研究入组时的疾病日而有所不同。
在 5642 例确诊的登革热病例中,我们确定了 259 例(4.6%)重症登革热病例、701 例(12.4%)血浆渗漏患者和 4008 例(40.0%)在门诊招募的患者中随后住院的患者。从发热早期开始,更高的病毒血症增加了发生所有 3 个终点的风险,但与二次免疫反应的影响相比,影响程度较小(每增加 1 个对数增加 1.12-1.27 的 OR)。这些关联在年龄、血清型和免疫状态组以及我们进行的各种敏感性和亚组分析中是一致的。
无论血清型或免疫状态如何,较高的血浆病毒血症与登革热严重程度的增加相关。