Center for Clinical Management Research, VA Ann Arbor Healthcare System, Ann Arbor, Michigan; University of Michigan School of Public Health, Ann Arbor, Michigan.
The Pulmonary Center, Boston University School of Medicine, Boston, Massachusetts; Center for Healthcare Organization and Implementation Research, Edith Nourse Rogers Memorial Veterans Hospital, Bedford, Massachusetts.
Am J Prev Med. 2021 Apr;60(4):520-528. doi: 10.1016/j.amepre.2020.10.014. Epub 2020 Dec 17.
Little is known about how clinicians make low-dose computed tomography lung cancer screening decisions in practice. Investigators assessed the factors associated with real-world decision making, hypothesizing that lung cancer risk and comorbidity would not be associated with agreeing to or receiving screening. Though these factors are key determinants of the benefit of lung cancer screening, they are often difficult to incorporate into decisions without the aid of decision tools.
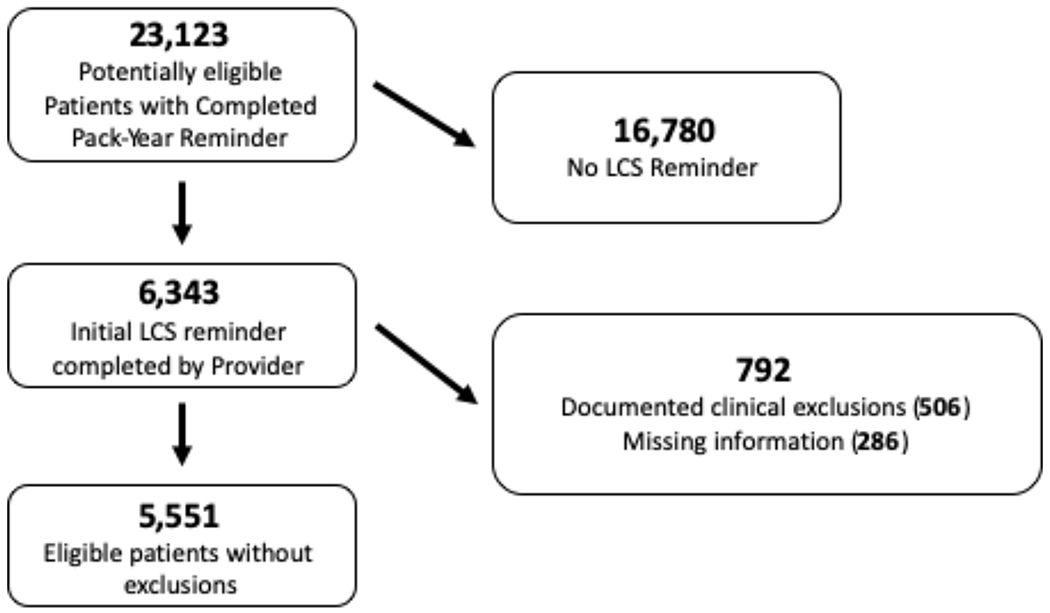
This was a retrospective cohort study of patients meeting current national eligibility criteria and deemed appropriate candidates for lung cancer screening on the basis of clinical reminders completed over a 2-year period (2013-2015) at 8 Department of Veterans Affairs medical facilities. Multilevel mixed-effects logistic regression models (conducted in 2019-2020) assessed predictors (age, sex, lung cancer risk, Charlson Comorbidity Index, travel distance to facility, and central versus outlying decision-making location) of primary outcomes of agreeing to and receiving lung cancer screening.
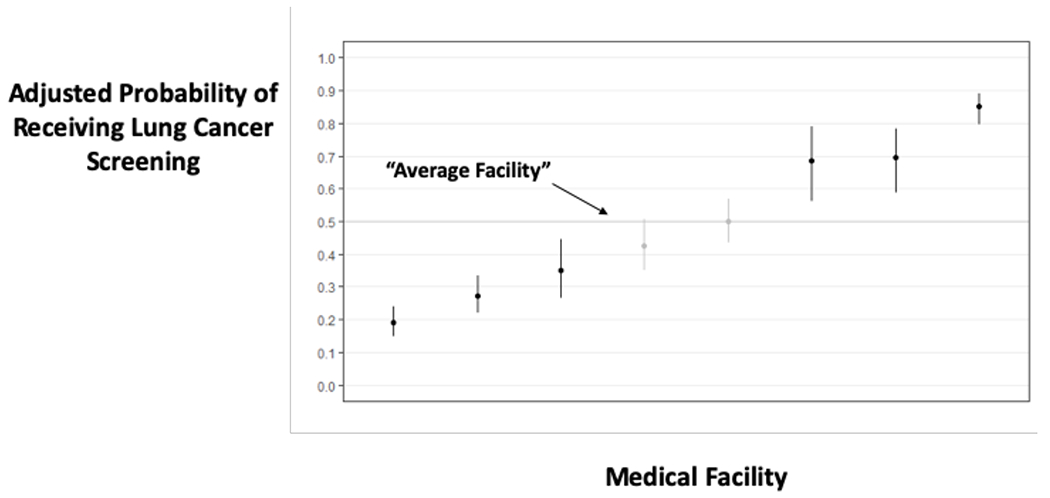
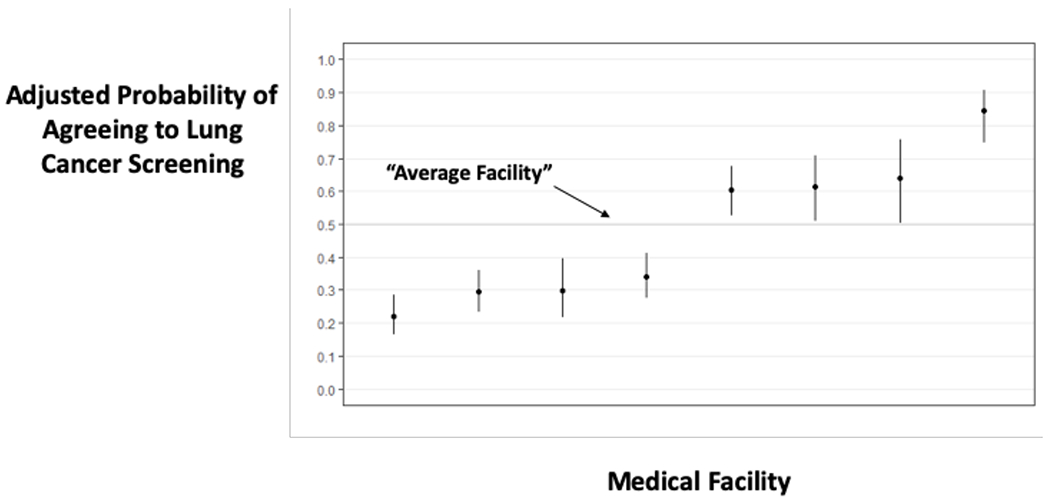
Of 5,551 patients (mean age=67 years, 97% male, mean lung cancer risk=0.7%, mean Charlson Comorbidity Index=1.14, median travel distance=24.2 miles), 3,720 (67%) agreed to lung cancer screening and 2,398 (43%) received screening. Lung cancer risk and comorbidity score were not strong predictors of agreeing to or receiving screening. Empirical Bayes adjusted rates of agreeing to and receiving screening ranged from 22% to 84% across facilities and from 19% to 85% across clinicians. A total of 33.7% of the variance in agreeing to and 34.2% of the variance in receiving screening was associated with the facility or the clinician offering screening.
Substantial variation was found in Veterans agreeing to and receiving lung cancer screening during the Veterans Affairs Lung Cancer Screening Demonstration Project. This variation was not explained by differences in key determinants of patient benefit, whereas the facility and clinician advising the patient had a large impact on lung cancer screening decisions.
关于临床医生在实践中如何做出低剂量计算机断层扫描肺癌筛查决策,我们知之甚少。研究人员评估了与实际决策相关的因素,假设肺癌风险和合并症与同意或接受筛查无关。尽管这些因素是肺癌筛查获益的关键决定因素,但如果没有决策工具的帮助,通常很难将这些因素纳入决策中。
这是一项回顾性队列研究,纳入了在 8 个退伍军人事务部医疗设施中在 2013 年至 2015 年期间完成的临床提醒,符合当前国家资格标准且被认为是肺癌筛查合适候选者的患者。多水平混合效应逻辑回归模型(于 2019-2020 年进行)评估了同意和接受肺癌筛查的主要结局的预测因素(年龄、性别、肺癌风险、Charlson 合并症指数、到设施的旅行距离以及中心与偏远决策地点)。
在 5551 名患者中(平均年龄 67 岁,97%为男性,平均肺癌风险 0.7%,平均 Charlson 合并症指数 1.14,中位数旅行距离 24.2 英里),3720 名(67%)同意进行肺癌筛查,2398 名(43%)接受了筛查。肺癌风险和合并症评分并不是同意或接受筛查的有力预测因素。在各个设施中,同意和接受筛查的经验贝叶斯调整率从 22%到 84%不等,在各个临床医生中从 19%到 85%不等。同意和接受筛查的方差中有 33.7%和 34.2%与提供筛查的设施或临床医生有关。
在退伍军人事务部肺癌筛查示范项目中,退伍军人同意和接受肺癌筛查的情况存在很大差异。这种差异不能用患者获益的关键决定因素的差异来解释,而设施和为患者提供建议的临床医生对肺癌筛查决策有很大影响。